Catching It Early: The Silent Warning Signs of Pancreatic Cancer
Learn the silent warning signs of pancreatic cancer, early symptoms, risk factors, diagnosis, and treatment options to improve the chances of early detection.
Introduction
Pancreatic cancer is often referred to as the “silent disease” since it starts developing without noticeable symptoms. The lack of early symptoms often leads to late diagnosis of this condition when the patient experiences pain or other complications associated with an already advanced stage of cancer development. Recognizing early warning signs and knowing about possible risk factors will allow diagnosing this cancer at the earliest stage, which would help a lot with choosing the best treatment strategy and increasing chances of successful recovery.
Even though pancreatic cancer is rather uncommon among all cancer types, this disease ranks among the most deadly cancerous conditions. Progress in medical sciences and new diagnostic methods, personalized treatments, and targeted therapies allow gradually improving survival rates for this type of cancer.
The current paper discusses in detail pancreatic cancer, including its causes, anatomy, symptoms, diagnosis, treatment, and the life of patients who deal with this disease.
What Is Pancreatic Cancer?
Pancreatic cancer represents a condition when some cells start growing uncontrollably and forming tumors in the pancreas. Cancerous cells not only invade surrounding tissues but may metastasize and affect other parts of the body, for example, liver, lungs, or abdomen.
The pancreas is an important organ placed behind the stomach. This organ serves two major functions:
- Production of enzymes that help to digest food
- Production of hormones, such as insulin and glucagon, that help to control the level of blood sugar
The appearance of cancer in the pancreas may influence both digestion and regulation of blood sugar levels.
One of the main features of pancreatic cancer is the absence of early symptoms.
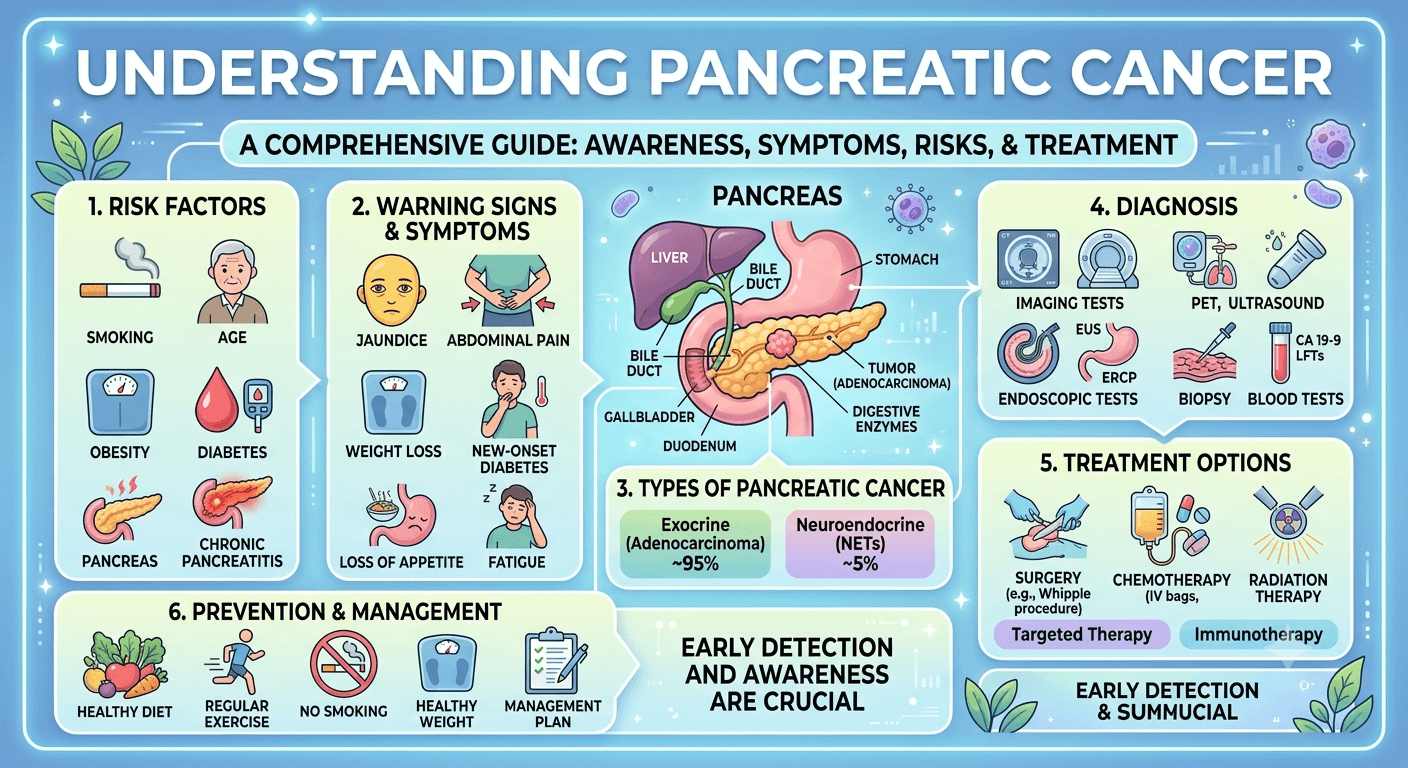
Types of Pancreatic Cancer
Pancreatic cancer is broadly classified into two major categories.
1. Exocrine Pancreatic Cancer
Approximately 90–95% of pancreatic cancers originate from the exocrine cells that produce digestive enzymes.
The most common type is:
Pancreatic Ductal Adenocarcinoma (PDAC)
- Begins in the ducts carrying digestive enzymes
- Most aggressive form
- Responsible for the majority of pancreatic cancer deaths
Other rare exocrine cancers include:
- Acinar cell carcinoma
- Adenosquamous carcinoma
- Squamous cell carcinoma
2. Neuroendocrine Pancreatic Tumors (PNETs)
These cancers develop from hormone-producing endocrine cells.
Some produce excessive hormones, causing noticeable symptoms, while others remain non-functional.
Examples include:
- Insulinomas
- Gastrinomas
- Glucagonomas
- VIPomas
Neuroendocrine tumors generally grow more slowly and often have a better prognosis than pancreatic adenocarcinoma.
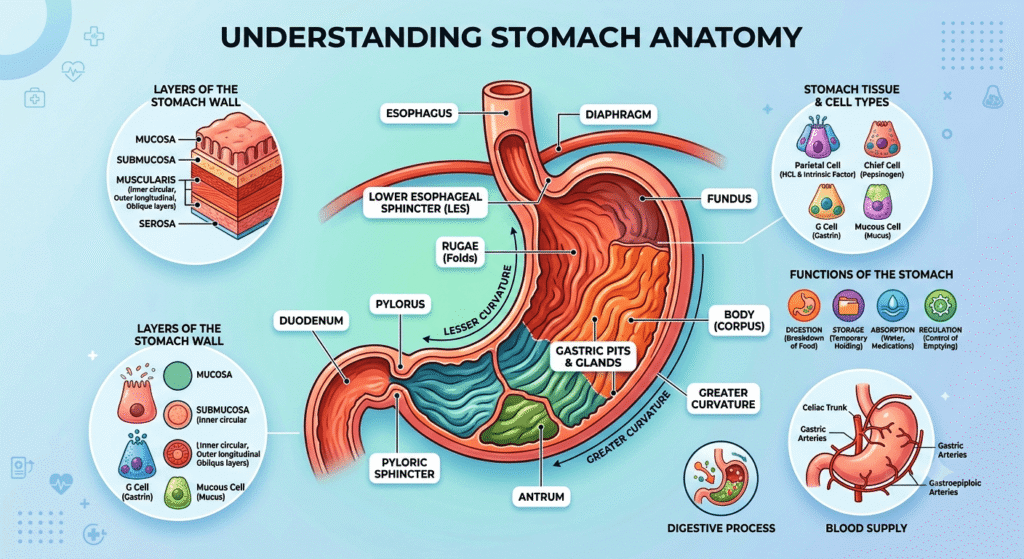
Anatomy of the Pancreas
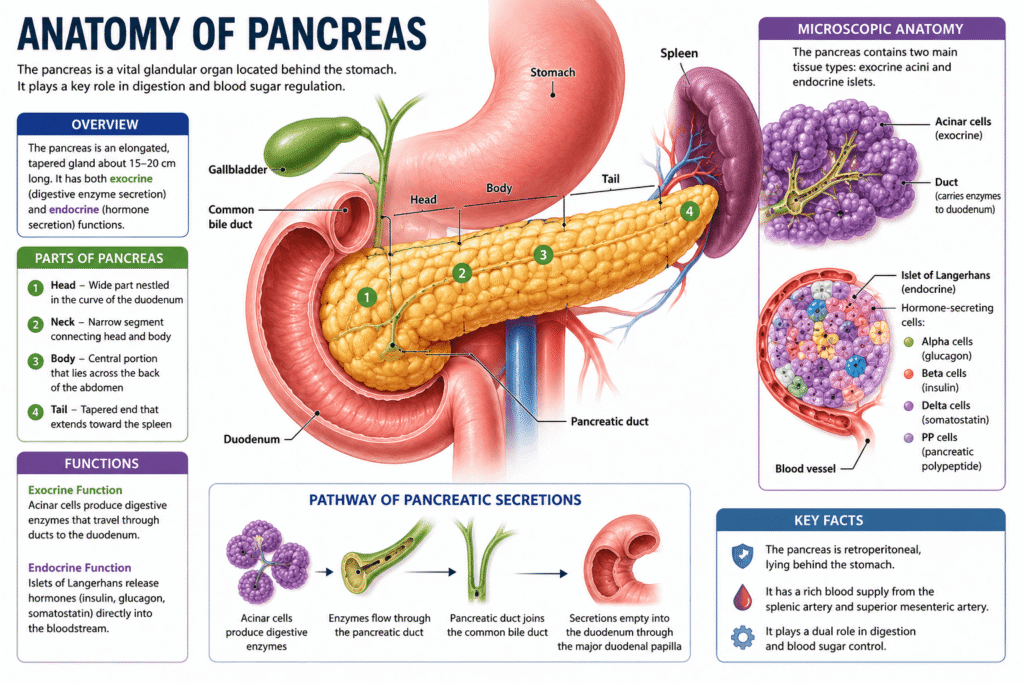
The pancreas is a long, flat gland measuring about 15–20 cm (6–8 inches) in length.
It consists of three major sections:
Head
- Located near the small intestine (duodenum)
- Most pancreatic cancers develop here
Body
- Middle portion extending across the abdomen
Tail
- Extends toward the spleen
- Tumors here are often detected later because they cause fewer early symptoms
Functions of the Pancreas
Exocrine Function
Produces digestive enzymes including:
- Amylase
- Lipase
- Proteases
These enzymes help digest carbohydrates, fats, and proteins.
Endocrine Function
Produces hormones including:
- Insulin
- Glucagon
- Somatostatin
These regulate blood glucose and metabolism.
Pathophysiology
Pancreatic cancer develops through a gradual accumulation of genetic mutations that transform healthy pancreatic cells into malignant ones.
The process often begins with precancerous lesions known as:
- PanIN (Pancreatic Intraepithelial Neoplasia)
- IPMN (Intraductal Papillary Mucinous Neoplasm)
- MCN (Mucinous Cystic Neoplasm)
Over time, mutations in genes such as:
- KRAS
- TP53
- CDKN2A
- SMAD4
allow cells to:
- Divide uncontrollably
- Resist normal cell death
- Invade nearby tissues
- Spread through blood vessels and lymphatics
Pancreatic tumors also create a dense fibrous environment that limits blood supply and makes chemotherapy less effective.
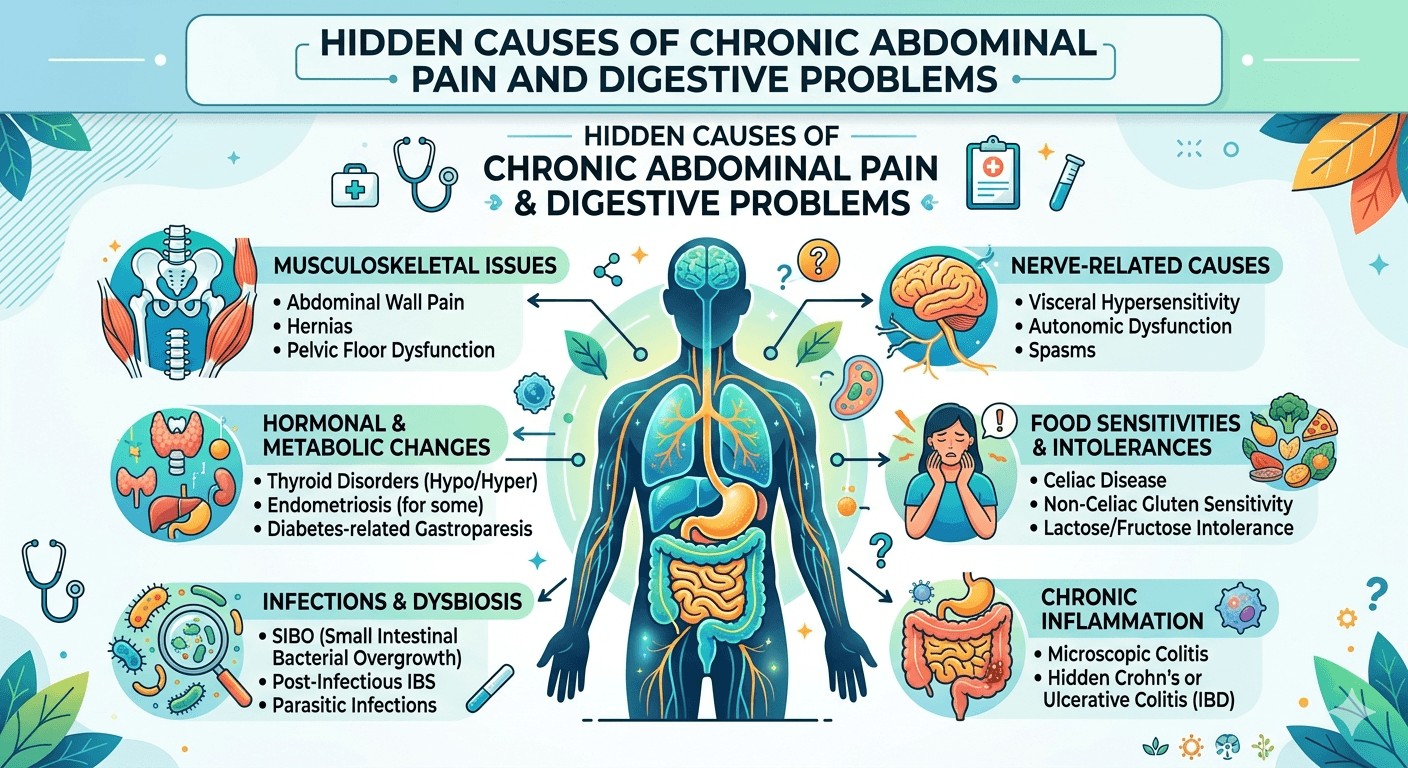
Silent Warning Signs of Pancreatic Cancer
One reason pancreatic cancer is so dangerous is that symptoms may initially seem mild or unrelated.
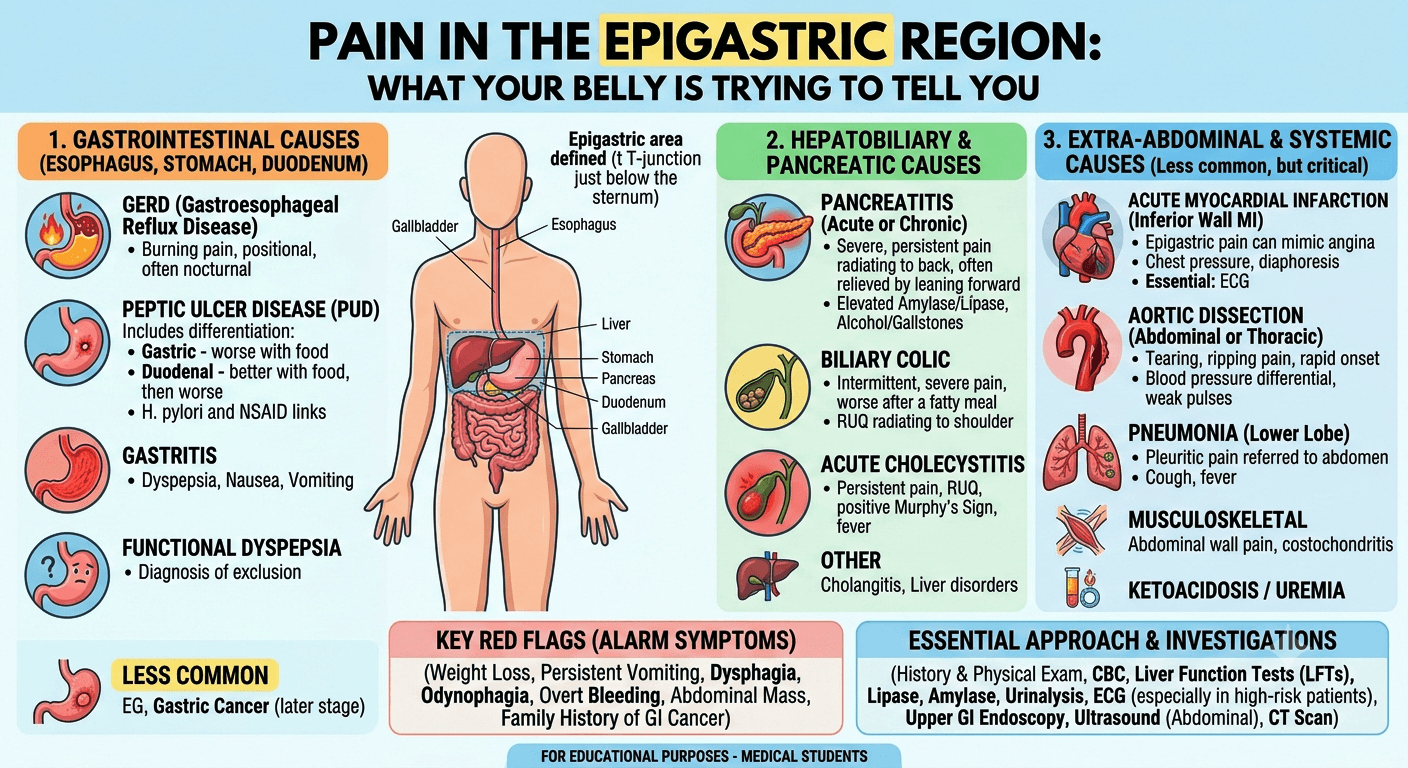
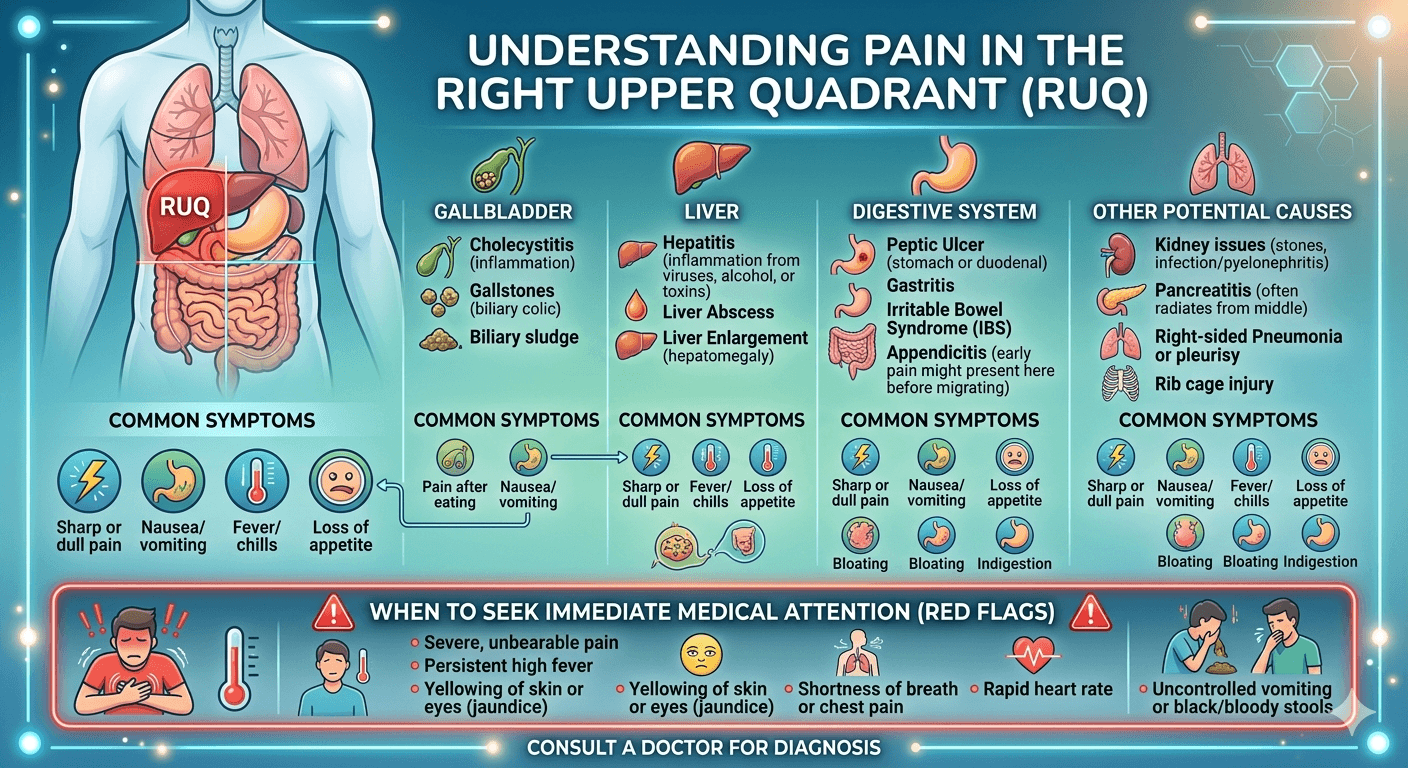
Persistent Upper Abdominal Pain
Pain often develops in the upper abdomen and may radiate to the back.
It may worsen:
- After eating
- While lying flat
Unexplained Weight Loss
Unexpected weight loss is one of the earliest warning signs.
Patients often notice:
- Loss of appetite
- Feeling full quickly
- Muscle wasting
Jaundice
Tumors in the pancreatic head can block the bile duct.
Symptoms include:
- Yellow skin
- Yellow eyes
- Dark urine
- Pale stools
- Itchy skin
Digestive Problems
Many patients develop:
- Nausea
- Vomiting
- Indigestion
- Bloating
- Fatty stools
- Diarrhea
New-Onset Diabetes
Suddenly developing diabetes after age 50 without obvious risk factors can occasionally be an early indicator of pancreatic cancer.
Fatigue
Persistent tiredness often accompanies cancer progression.
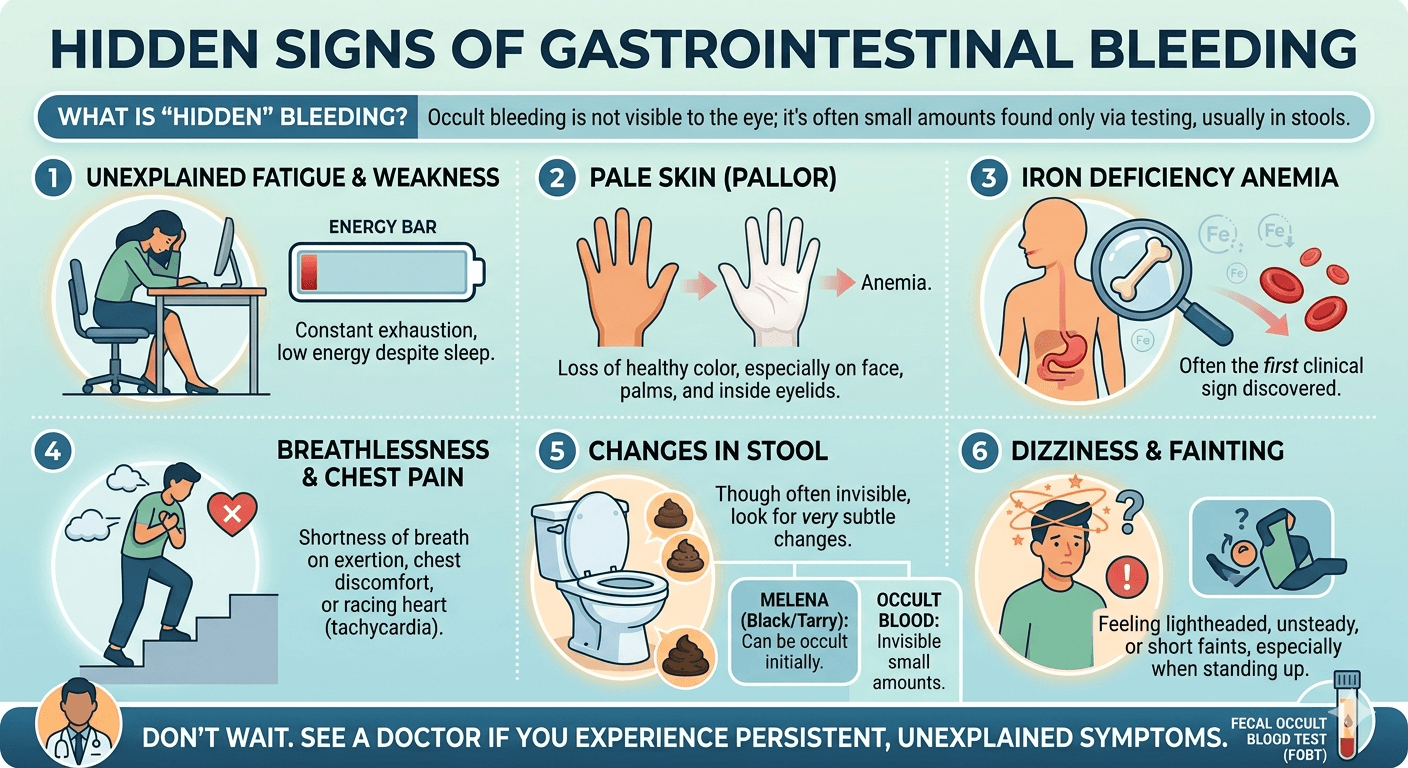
Blood Clots
Some patients experience unexplained blood clots before their cancer diagnosis.
Back Pain
Pain spreading into the middle or lower back may occur as tumors enlarge.
Causes and Risk Factors
The exact cause of pancreatic cancer is not always known. It develops when genetic mutations cause pancreatic cells to grow uncontrollably, forming a tumor. Several lifestyle, environmental, and inherited factors can increase the risk of developing the disease.
Common risk factors include:
- Smoking: The leading preventable risk factor, significantly increasing the likelihood of pancreatic cancer.
- Older age: Most cases occur in people over 60 years of age.
- Family history: Having close relatives with pancreatic cancer raises the risk.
- Inherited genetic syndromes: Mutations in genes such as BRCA1, BRCA2, PALB2, CDKN2A, STK11, and PRSS1 can increase susceptibility.
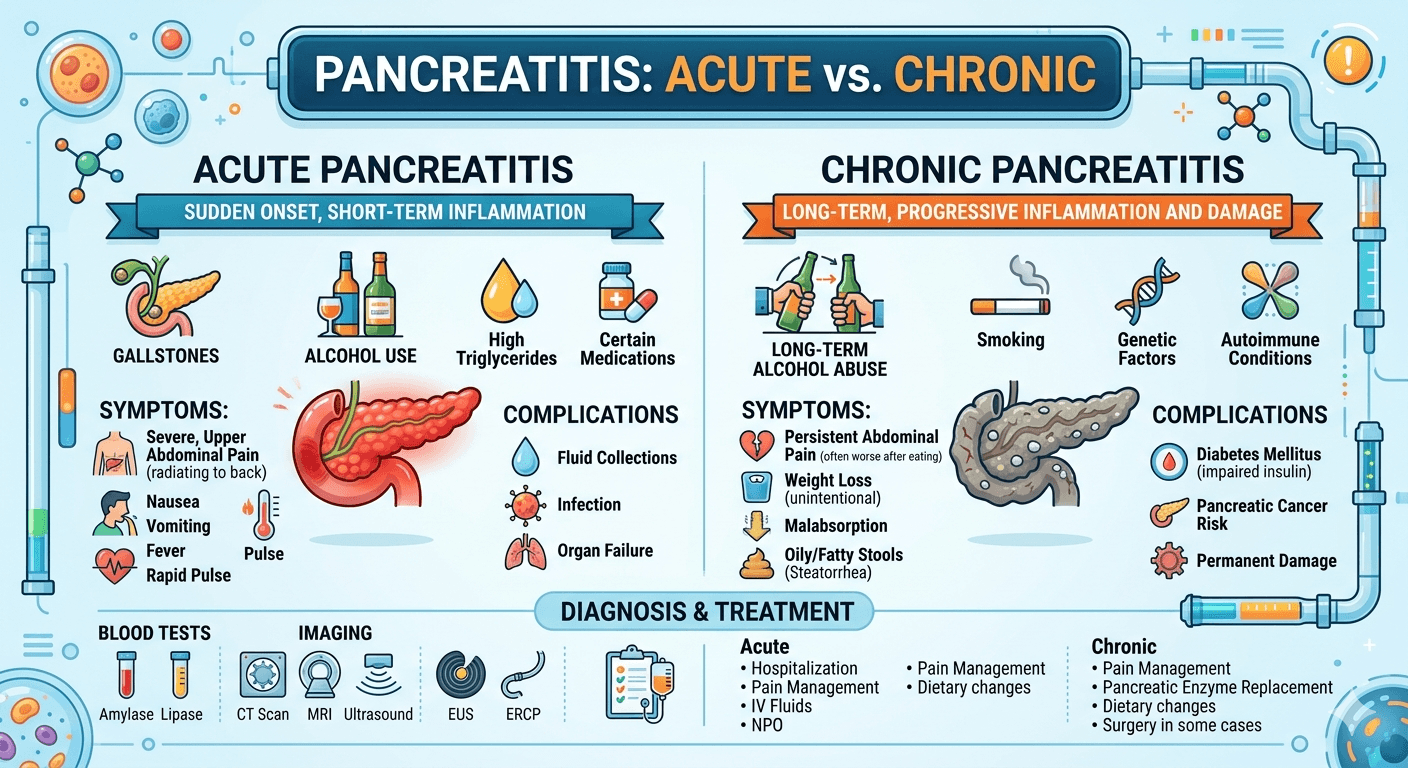
- Chronic pancreatitis: Long-term inflammation of the pancreas increases cancer risk, particularly hereditary pancreatitis.
- Diabetes mellitus: Long-standing type 2 diabetes and newly diagnosed diabetes in older adults may be associated with pancreatic cancer.
- Obesity: Excess body weight contributes to chronic inflammation and metabolic changes that promote cancer development.
- Unhealthy diet: Diets high in processed meats, red meat, and saturated fats and low in fruits and vegetables may increase risk.
- Heavy alcohol consumption: Excessive alcohol intake can lead to chronic pancreatitis, an established risk factor.
- Physical inactivity: A sedentary lifestyle contributes indirectly through obesity and insulin resistance.
- Occupational exposure: Long-term exposure to certain chemicals used in the petroleum, metalworking, and pesticide industries may increase risk.
- Race and ethnicity: Incidence is higher in some populations, including people of African ancestry.
- Male sex: Men have a slightly higher risk than women, partly due to higher rates of smoking and occupational exposures.
Diagnosis
Because symptoms are often vague, multiple diagnostic tools are used.
Medical History and Physical Examination
Doctors evaluate:
- Symptoms
- Weight changes
- Family history
- Risk factors
Blood Tests
May include:
- Liver function tests
- RBS, HbA1c
- CRP, ESR
- Kidney function test
- S. Amylase and S. Lipase
- Blood sugar levels
- CA 19-9 tumor marker
CA 19-9 alone cannot diagnose pancreatic cancer but helps monitor treatment.
Imaging Studies
Common imaging tests include:
- CT scan
- MRI
- MRCP
- PET scan
- Ultrasound
Endoscopic Ultrasound (EUS)
Allows detailed imaging while obtaining tissue samples through biopsy.
Biopsy
A biopsy confirms the diagnosis by examining tissue under a microscope.
Treatment Options
Treatment depends on:
- Stage
- Tumor location
- Overall health
- Cancer type
Surgery
Surgery offers the best chance for cure when cancer is localized.
Common procedures include:
Whipple Procedure
Removes:
- Pancreatic head
- Duodenum
- Gallbladder
- Part of the bile duct
Distal Pancreatectomy
Removes:
- Pancreatic body
- Tail
- Sometimes the spleen
Total Pancreatectomy
Entire pancreas removed.
Patients require lifelong insulin and digestive enzyme replacement.
Therapy
Chemotherapy
Common chemotherapy regimens include:
- FOLFIRINOX
- Gemcitabine
- Gemcitabine plus nab-paclitaxel
Chemotherapy may be given:
- Before surgery
- After surgery
- For advanced disease
Radiation Therapy
High-energy radiation destroys cancer cells.
It may:
- Shrink tumors
- Reduce pain
- Improve surgical outcomes
Targeted Therapy
Patients with specific genetic mutations may benefit from targeted medications.
Examples include:
- PARP inhibitors for BRCA mutations
- NTRK inhibitors for rare gene fusions
Immunotherapy
Although only effective in a small percentage of patients, immunotherapy can be beneficial for tumors with specific genetic characteristics such as mismatch repair deficiency.
Medications
Several medications help manage symptoms and improve quality of life.
These include:
Pain medications
- Acetaminophen
- NSAIDs
- Opioids
Pancreatic enzyme replacement
Improves digestion and nutrient absorption.
Insulin
For diabetes caused by pancreatic dysfunction.
Anti-nausea medications
Help reduce chemotherapy-related nausea.
Appetite stimulants
May improve nutritional intake.
Anticoagulants
Used if blood clots develop.
Living with Pancreatic Cancer
The condition influences one’s physical, psychological, social and economic aspects of life. However, people are able to live an enriched life, retain their connections and relationships, and feel well with proper treatment and assistance.
Eating Right
It is hard to eat properly due to problems with digestion and lack of appetite.
Useful measures comprise:
- Eating frequently and in small portions
- Foods with high amount of protein
- Taking pancreatic enzyme preparations
- Hydration
- Meeting with a nutritionist
Dealing with Fatigue
Fatigue is a typical problem.
There are some things that patients may find useful:
- Smooth physical activity
- Getting enough rest
- Conserving energy
- Balanced nutrition
Being Mentally Healthy
Anxiety, sadness, or fear may be felt. One may use counseling services, take part in discussion groups, engage in meditation and speak to relatives and friends.
Palliative Treatment
It helps to alleviate symptoms, control pain, and improve life quality. It can be used not only when cancer is terminal but also alongside active treatment.
Regular Check-Ups
They help to evaluate one’s progress in treatment, handle side effects and detect early signs of disease recurrence.
Frequently Asked Questions (FAQs)
Is pancreatic cancer hereditary?
Most cases are not inherited, but approximately 10% are associated with inherited genetic mutations or strong family history.
Can pancreatic cancer be cured?
When detected early and completely removed surgically, some patients can achieve long-term survival. However, many cases are diagnosed at an advanced stage.
Who is most at risk?
People over 60 years of age, smokers, individuals with obesity, chronic pancreatitis, diabetes, or a family history of pancreatic cancer have a higher risk.
Does pancreatic cancer always cause pain?
No. Early pancreatic cancer may not cause pain or any noticeable symptoms.
Can lifestyle changes reduce risk?
Maintaining a healthy weight, avoiding tobacco, limiting alcohol consumption, eating a balanced diet, and staying physically active may reduce the risk.
What are the survival rates?
Survival depends on the stage at diagnosis. Patients diagnosed when the disease is localized generally have significantly better outcomes than those diagnosed after the cancer has spread.
Conclusion
Pancreatic cancer continues to be one of the toughest cancers because it develops subtly with symptoms that could be misunderstood as something else. However, increased awareness of its hidden signs including sudden weight loss, constant abdominal or back pain, yellow skin or eyes, digestive problems, and diabetes could help people visit their doctor earlier and perhaps even save their lives.
With the development of better surgical procedures, chemotherapies, radiation therapies, targeted therapies, supportive care, and personalized medicine, many people are surviving longer. Nutritional support, pain relief, mental counseling, and palliative care are equally important during treatment.
If you have symptoms or some risk factors for developing the disease, it is crucial to visit your doctor without delay. Early detection, timely diagnosis, and comprehensive treatment are the best way of fighting this type of cancer.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment.