Learn about Kidney Failure Treatment, including causes, diagnosis, medications, dialysis, and transplant options to help protect kidney health.
Introduction
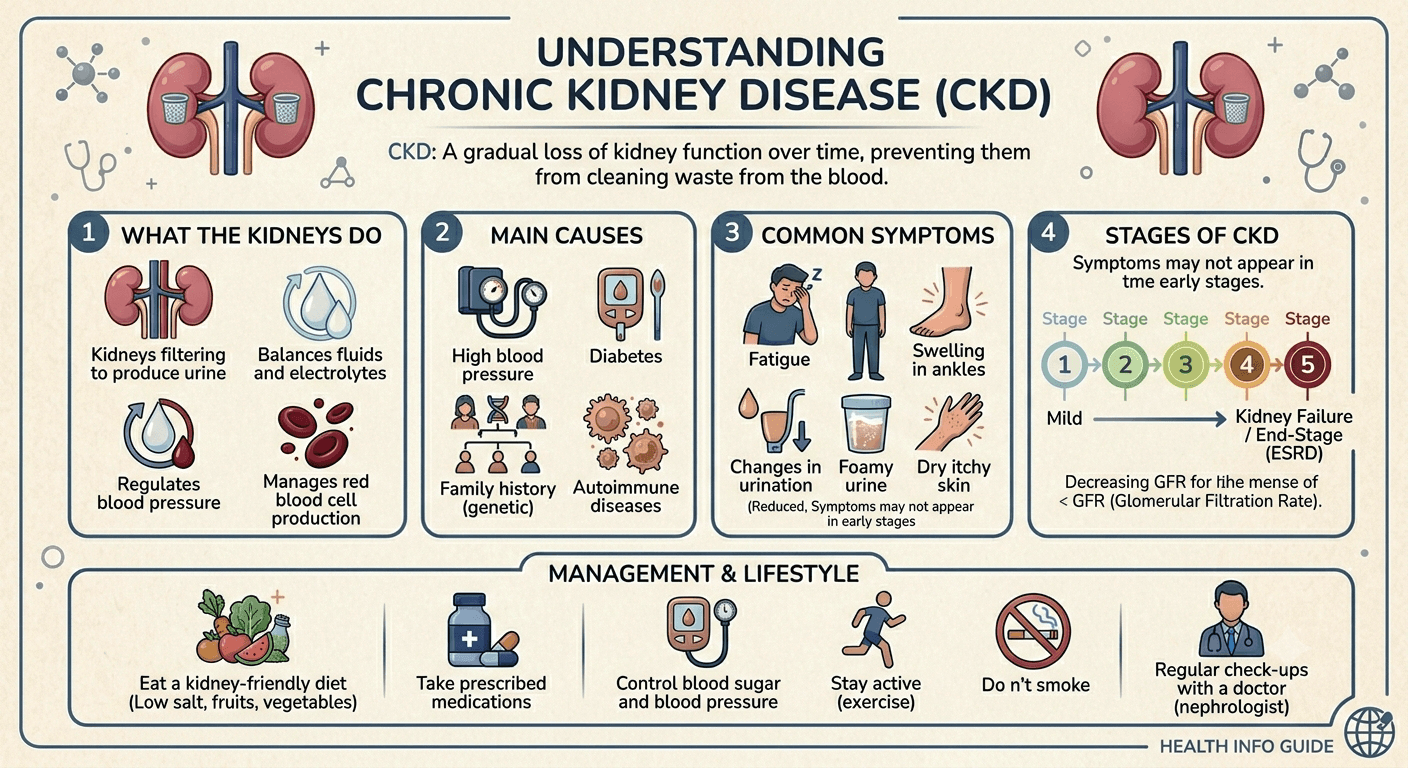
Kidney failure is a serious condition that occurs when the kidneys can no longer effectively filter waste products, excess fluid, and toxins from the blood. It may develop suddenly or progress gradually over time, often as a result of underlying conditions such as diabetes, high blood pressure, or chronic kidney disease. Early diagnosis and prompt treatment are essential to slow disease progression, prevent complications, and improve quality of life. In this guide, you’ll learn about the causes of kidney failure, how it is diagnosed, and the treatment options available, including medications, dialysis, kidney transplantation, and lifestyle changes.
In this comprehensive guide learn about Kidney Failure Treatment, including causes, diagnosis, medications, dialysis, and transplant options to help protect kidney health.
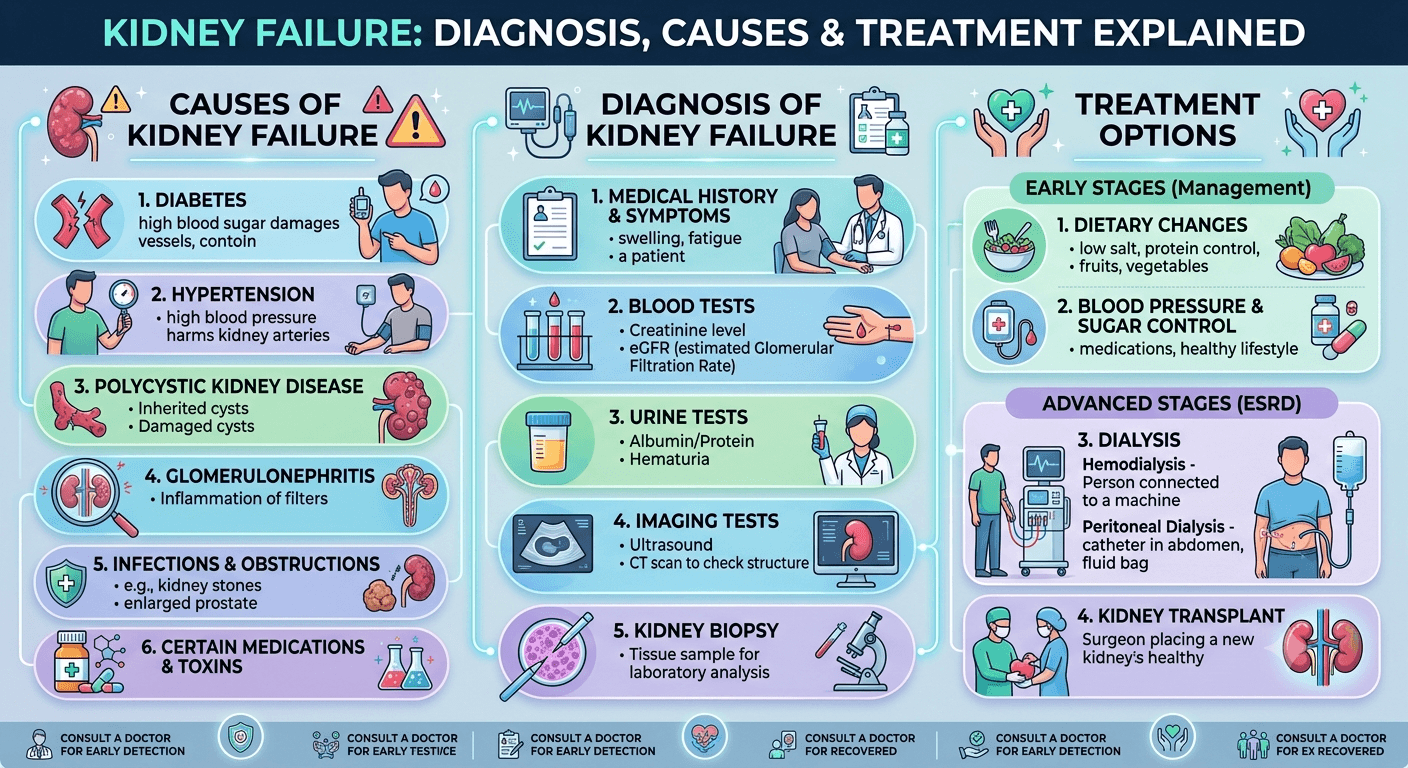
Causes and Risk Factors of Kidney Failure
Kidney failure rarely occurs without an underlying cause. In most cases, it develops as a result of chronic diseases that gradually damage the kidneys over many years or from acute conditions that suddenly impair kidney function. Identifying the cause is essential because early intervention can slow disease progression, prevent complications, and improve long-term outcomes.
1. Diabetes Mellitus
Diabetes is the leading cause of chronic kidney disease (CKD) and kidney failure worldwide.
Persistently elevated blood glucose damages the tiny blood vessels (glomeruli) responsible for filtering blood. Over time, this condition known as diabetic nephropathy reduces the kidneys’ filtering capacity, allowing protein to leak into the urine and eventually leading to irreversible kidney damage.
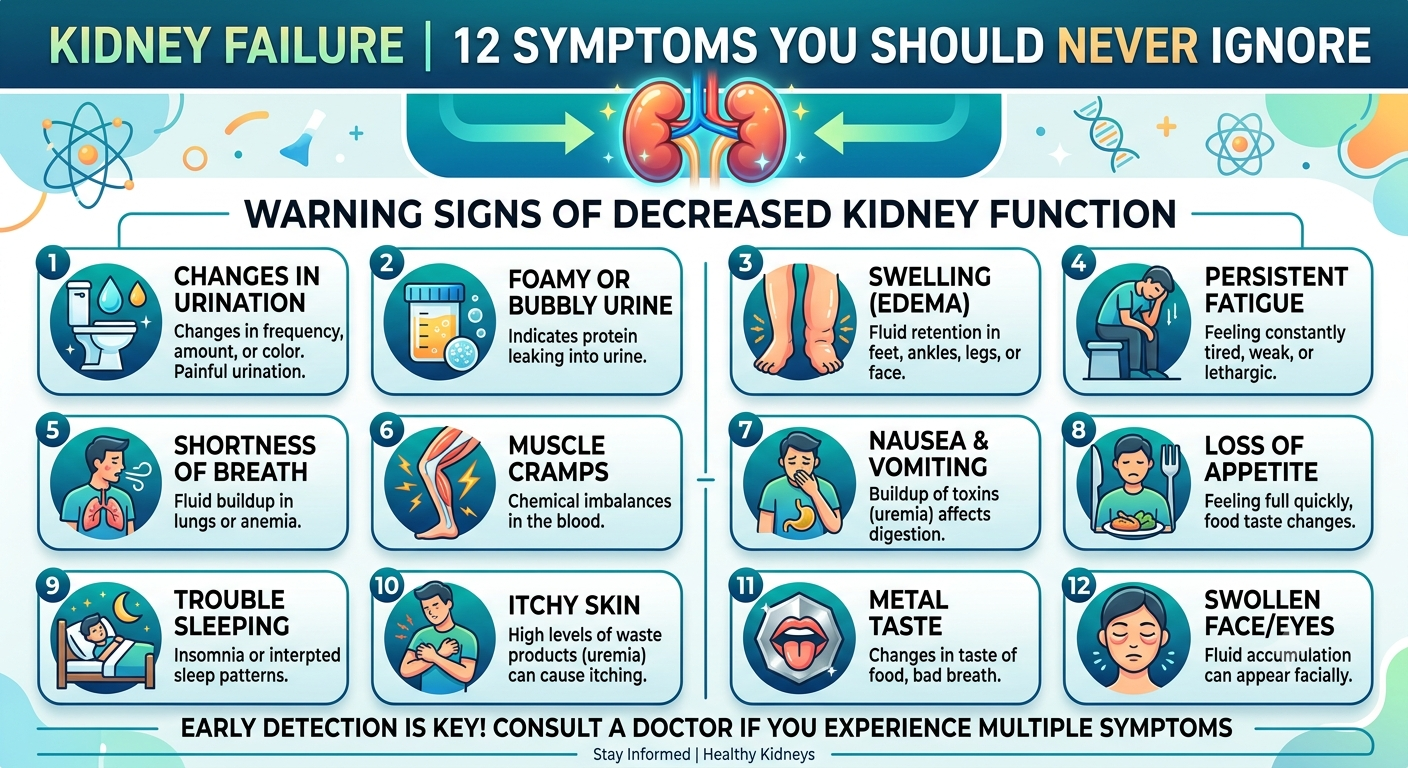
Warning signs include:
- Protein in the urine (albuminuria)
- Swelling of the feet
- Rising blood pressure
- Gradual decline in kidney function
Maintaining good blood sugar control significantly lowers the risk of diabetic kidney disease.
2. High Blood Pressure (Hypertension)
High blood pressure (Hypertension) is both a cause and a consequence of kidney disease.
Persistently elevated blood pressure damages the delicate blood vessels inside the kidneys, reducing their ability to filter blood effectively. As kidney function declines, blood pressure often becomes even more difficult to control, creating a harmful cycle of progressive damage.
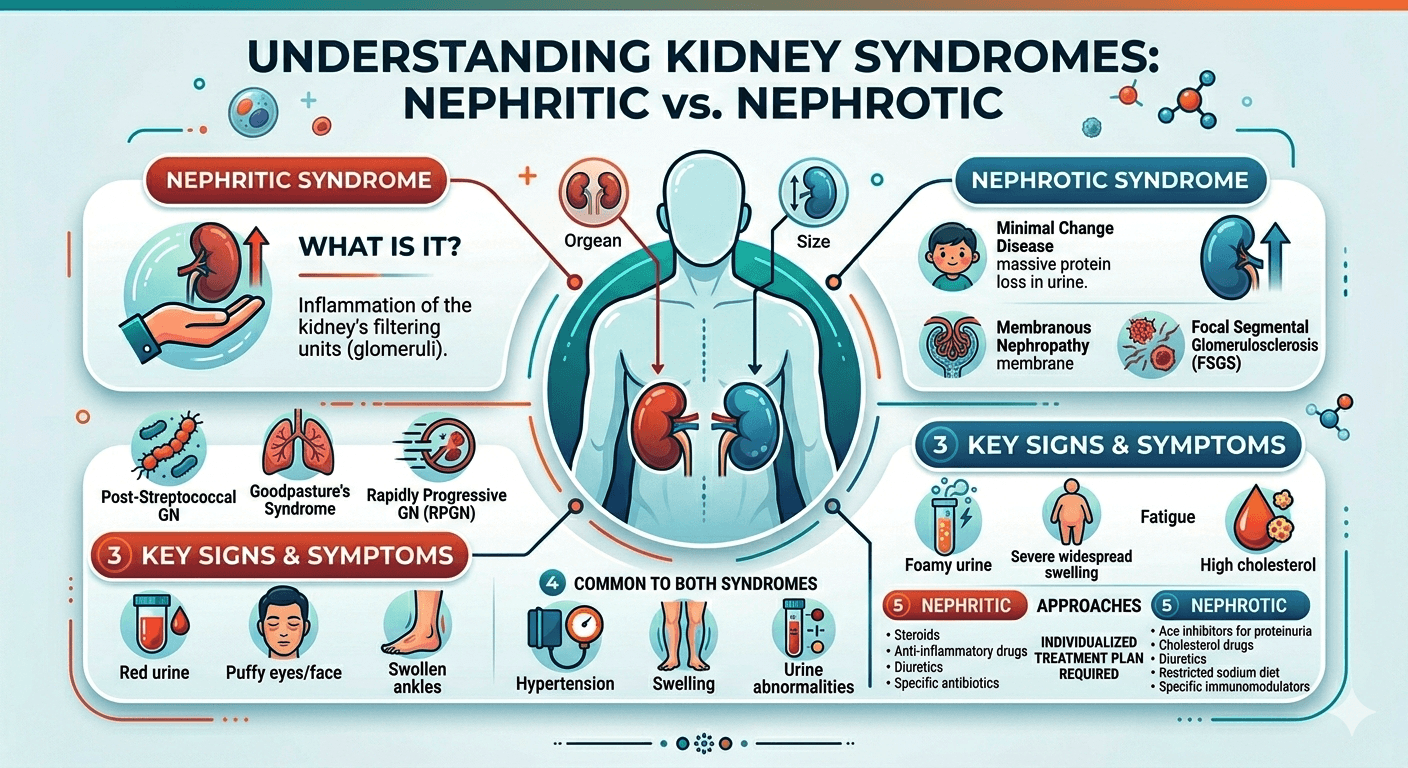
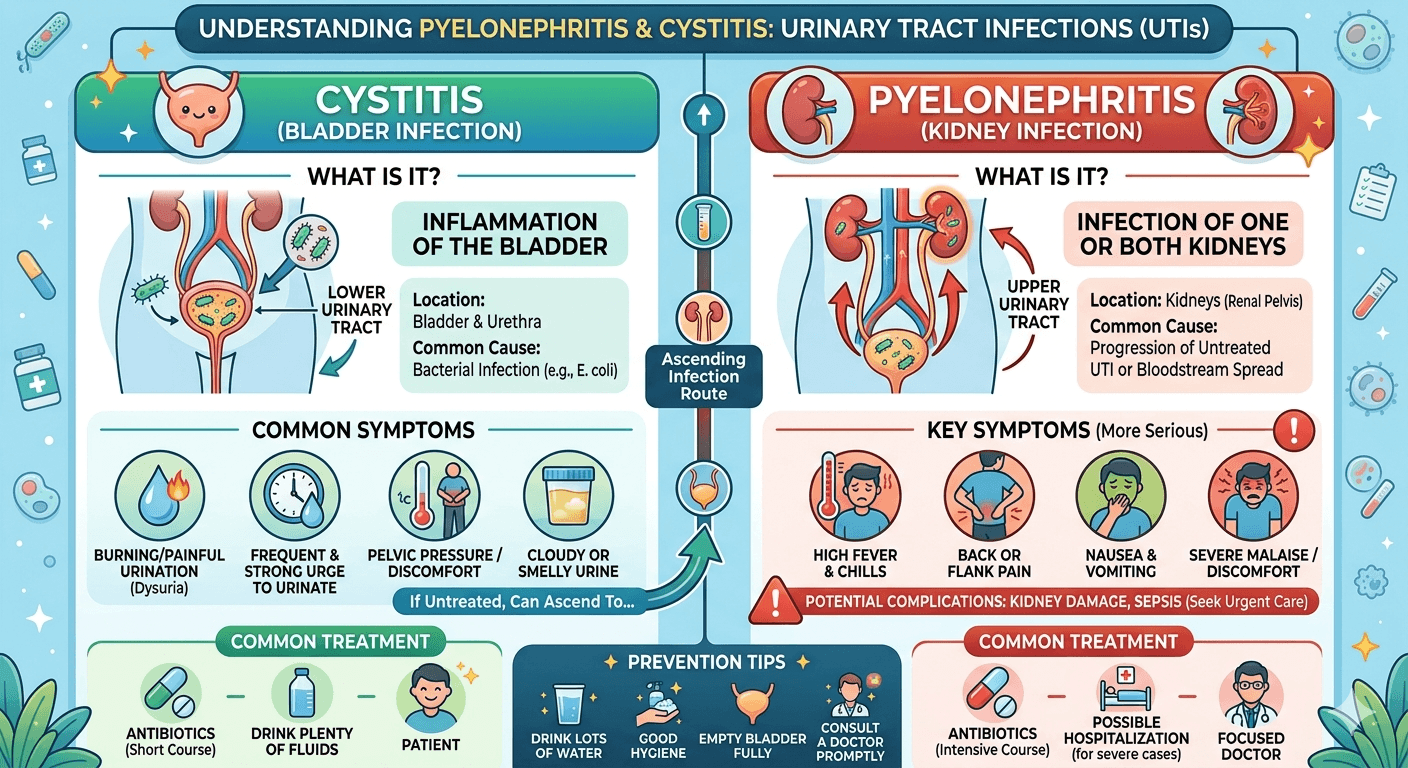
3. Glomerulonephritis
Glomerulonephritis refers to inflammation of the glomeruli, the tiny filtering units of the kidneys.
It may result from:
- Autoimmune diseases
- Infections
- Certain medications
- Genetic disorders
Patients may experience:
- Blood in the urine
- Foamy urine
- Swelling
- High blood pressure
Early diagnosis and treatment can help preserve kidney function.
4. Polycystic Kidney Disease (PKD)
Polycystic kidney disease is an inherited disorder characterized by the development of numerous fluid-filled cysts within the kidneys. Over time, these cysts enlarge, replacing healthy kidney tissue and impairing kidney function.
Symptoms may include:
- Flank pain
- Blood in the urine
- Kidney stones
- High blood pressure
- Enlarged kidneys
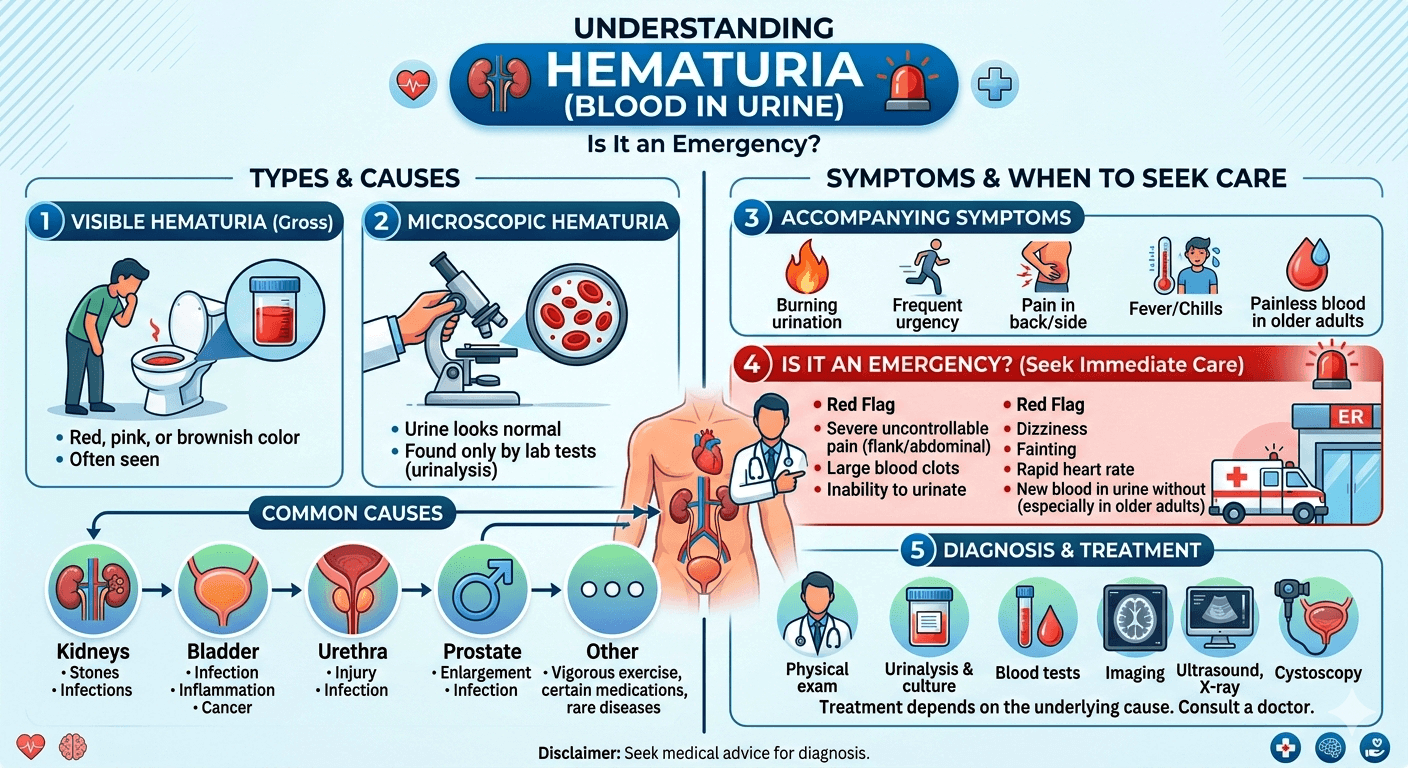
5. Urinary Tract Obstruction
Any blockage that prevents urine from flowing normally can damage the kidneys if left untreated.
Common causes include:
- Kidney stones
- Enlarged prostate
- Bladder tumors
- Urethral strictures
- Certain cancers
Prompt relief of the obstruction often improves kidney function.
6. Autoimmune Diseases
Several autoimmune conditions can attack the kidneys directly, including:
- Systemic lupus erythematosus (SLE)
- IgA nephropathy
- Vasculitis
- Goodpasture syndrome
These disorders cause inflammation that gradually damages kidney tissue.
7. Severe Infections (Sepsis)
Life-threatening infections can dramatically reduce blood flow to the kidneys and trigger acute kidney injury.
Sepsis remains one of the most common causes of acute kidney failure in hospitalized patients.
8. Certain Medications
Long-term or inappropriate use of certain medications may harm the kidneys, including:
- Nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen
- Certain antibiotics
- Some chemotherapy drugs
- Contrast dyes used during imaging studies
- Certain herbal supplements
Medications should always be taken as directed by a healthcare professional, especially in individuals with existing kidney disease.
9. Heart and Liver Diseases
Conditions that reduce blood flow to the kidneys can contribute to kidney failure, including:
- Heart failure
- Severe liver disease (cirrhosis)
- Cardiogenic shock
10. Dehydration
Severe dehydration caused by prolonged vomiting, diarrhea, excessive sweating, or inadequate fluid intake can reduce blood flow to the kidneys, leading to acute kidney injury if not corrected promptly.
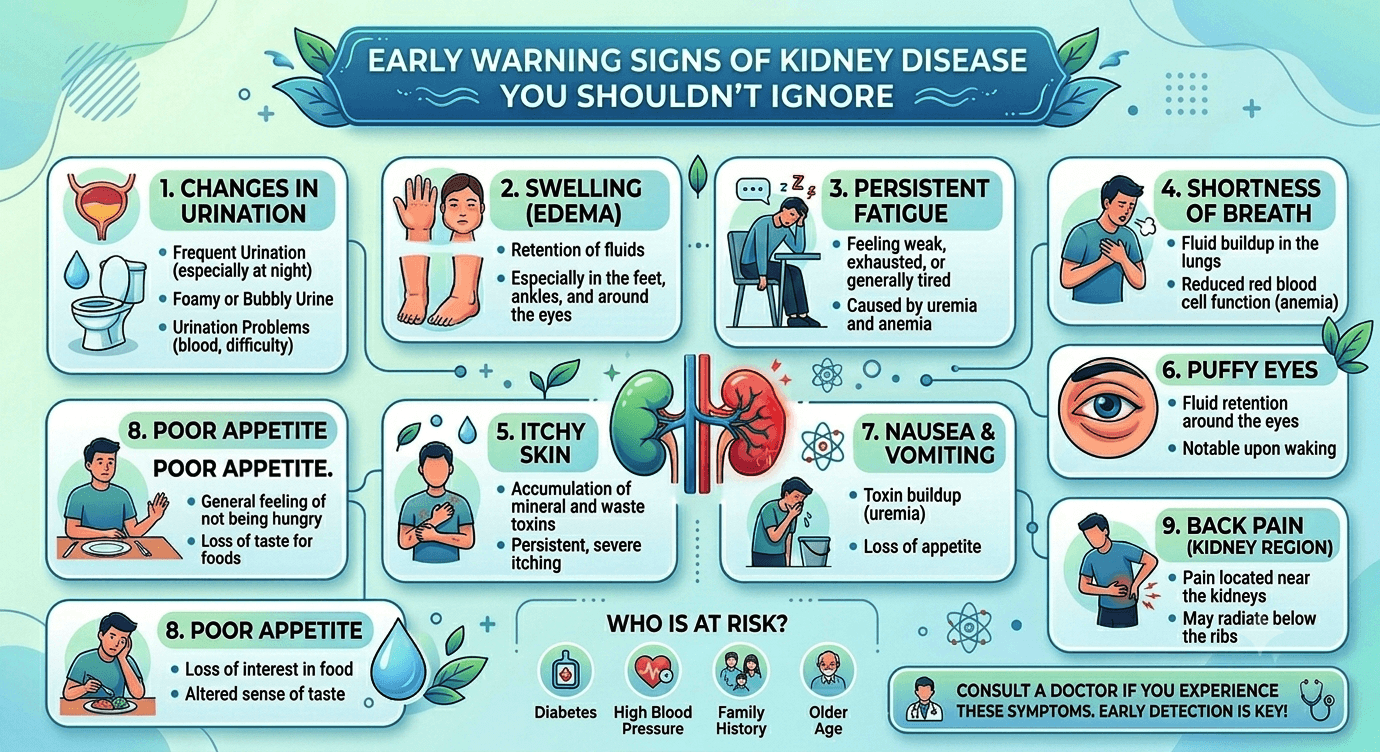
Who Is at Higher Risk?
Several factors increase the likelihood of developing kidney failure:
- Age over 60 years
- Diabetes mellitus
- High blood pressure
- Cardiovascular disease
- Family history of kidney disease
- Obesity
- Smoking
- Chronic use of pain-relieving medications
- Autoimmune disorders
- Recurrent urinary tract infections
- Kidney stones
- African, Hispanic, Native American, and certain Asian populations have a higher prevalence of chronic kidney disease due to a combination of genetic, environmental, and socioeconomic factors.
People with these risk factors should undergo regular kidney function screening.
Diagnosis of Kidney Failure
Early diagnosis allows healthcare providers to slow disease progression, manage complications, and improve quality of life.
Medical History
The physician will ask about:
- Symptoms
- Family history
- Diabetes
- Hypertension
- Medication use
- Previous kidney disease
- Recent infections
- Fluid intake and urine output
Physical Examination
The healthcare provider evaluates:
- Blood pressure
- Swelling (edema)
- Weight changes
- Heart and lung sounds
- Signs of dehydration
- Skin changes
- Neurological status
Blood Tests
- Kidney function test
- CBC
- LDH
- Lipid profile
- Diabetic panel (RBS, HbA1c, INSULIN)
Serum Creatinine
Creatinine is a waste product produced by muscles.
Elevated creatinine usually indicates reduced kidney function.
Estimated Glomerular Filtration Rate (eGFR)
The eGFR estimates how efficiently the kidneys filter blood.
General interpretation:
| eGFR (mL/min/1.73 m²) | Kidney Function |
| 90 or above | Normal |
| 60–89 | Mild decrease |
| 30–59 | Moderate CKD |
| 15–29 | Severe CKD |
| Below 15 | Kidney failure |
Blood Urea Nitrogen (BUN)
High BUN levels often indicate reduced kidney function but can also rise due to dehydration or gastrointestinal bleeding.
Electrolyte Panel
Tests measure:
- Potassium
- Sodium
- Calcium
- Phosphate
- Bicarbonate
Abnormal values help guide treatment.
Urine Tests
Urinalysis evaluates:
- Protein
- Blood
- Infection
- Glucose
- Microscopic abnormalities
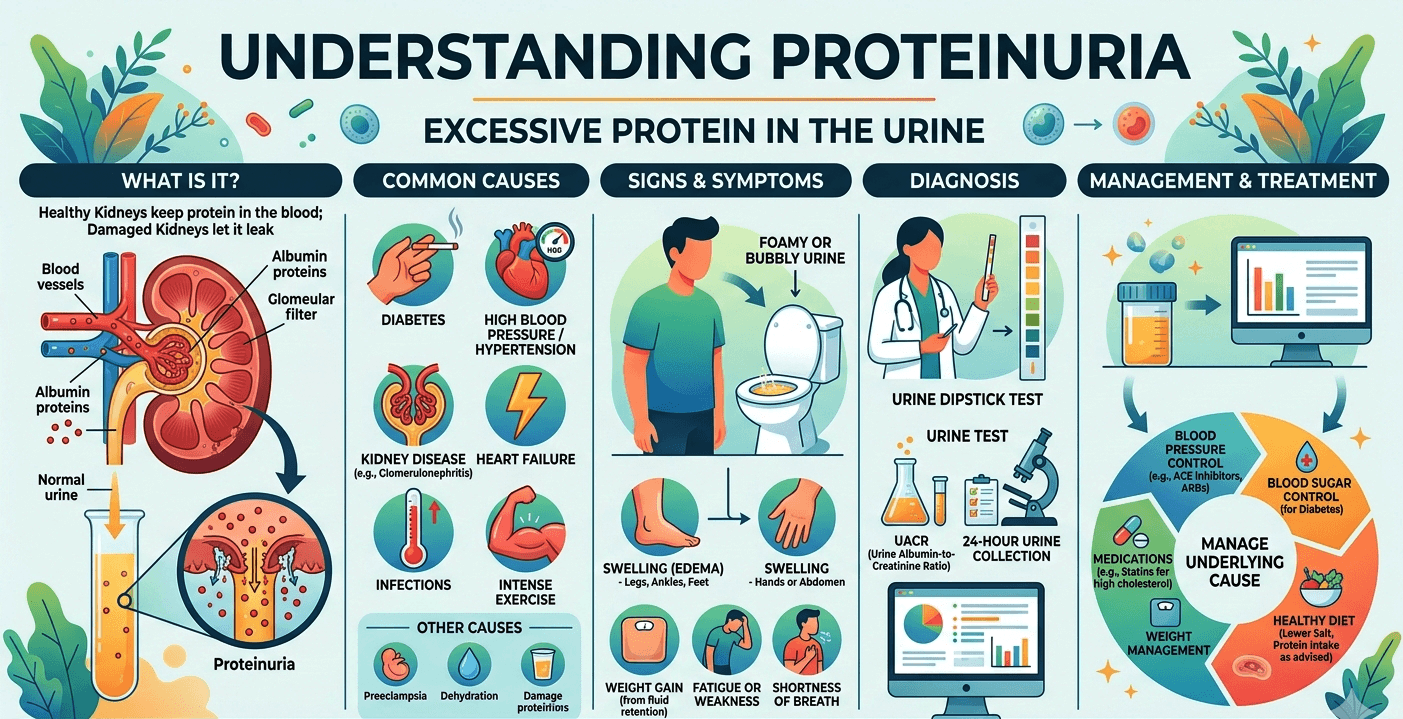
Urine Albumin-to-Creatinine Ratio (UACR)
One of the earliest indicators of kidney damage is excess albumin in the urine, particularly in people with diabetes or hypertension.
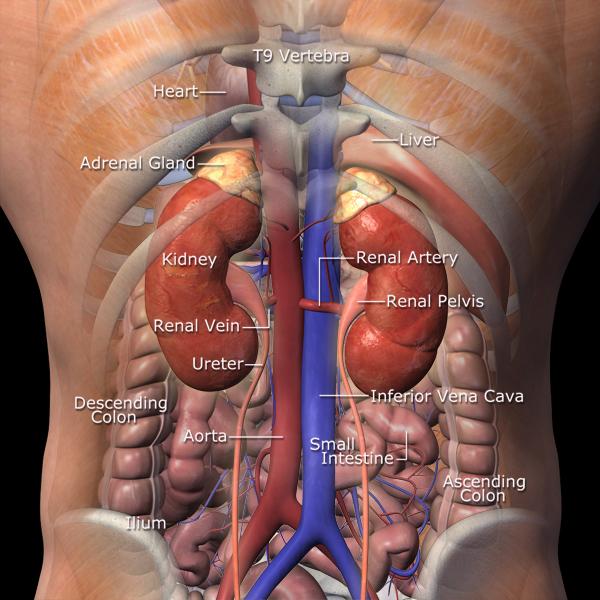
Imaging Studies
Imaging helps evaluate kidney size, structure, and blood flow.
Common tests include:
- Kidney ultrasound
- CT scan
- MRI
- Doppler ultrasound
Kidney Biopsy
In selected patients, a small sample of kidney tissue is examined under a microscope to determine the exact cause of kidney disease.
Treatment Options for Kidney Failure
Treatment depends on:
- The underlying cause
- Whether kidney failure is acute or chronic
- The severity of kidney damage
- Overall health
- Associated medical conditions
The primary goals are to preserve remaining kidney function, manage symptoms, prevent complications, and improve quality of life.
1. Treating the Underlying Cause
Whenever possible, the underlying disease should be addressed.
Examples include:
- Improving blood sugar control in diabetes
- Managing high blood pressure
- Treating infections
- Relieving urinary obstruction
- Discontinuing nephrotoxic medications
- Treating autoimmune diseases with immunosuppressive therapy
2. Lifestyle Modifications
Lifestyle changes play a vital role in slowing the progression of chronic kidney disease.
Patients are encouraged to:
- Follow a kidney-friendly diet
- Limit sodium intake
- Avoid smoking
- Maintain a healthy weight
- Exercise regularly, as tolerated
- Stay adequately hydrated (following medical advice)
- Avoid unnecessary over-the-counter pain medications
3. Dietary Therapy (Medical Nutrition Therapy)
Nutrition is one of the most important components of kidney disease management. A renal dietitian can help create a personalized eating plan based on the stage of kidney disease and laboratory results.
Key dietary recommendations may include:
- Limiting sodium to help control blood pressure and reduce fluid retention.
- Adjusting protein intake to reduce the kidneys’ workload while maintaining adequate nutrition.
- Monitoring potassium intake if blood potassium levels are elevated.
- Limiting phosphorus-rich foods to protect bone health.
- Managing fluid intake in advanced kidney disease to prevent fluid overload.
Dietary needs vary significantly between individuals, particularly for those receiving dialysis, so professional guidance is essential.
Therapy for Kidney Failure
Treatment often extends beyond medications and includes supportive therapies aimed at preserving kidney function and improving overall health.
Blood Pressure Management
Strict blood pressure control is one of the most effective ways to slow kidney disease progression. Lifestyle measures combined with prescribed medications help protect the kidneys and reduce cardiovascular risk.
Blood Sugar Management
For people with diabetes, maintaining blood glucose within the target range helps prevent further damage to the kidneys.
Anemia Management
Reduced production of erythropoietin by damaged kidneys can lead to anemia. Treatment may include iron supplementation and erythropoiesis-stimulating agents (ESAs) under medical supervision.
Bone and Mineral Disorder Management
Chronic kidney disease can disrupt calcium, phosphorus, and vitamin D balance. Therapy may involve dietary changes, vitamin D supplements, and phosphate binders to protect bone health.
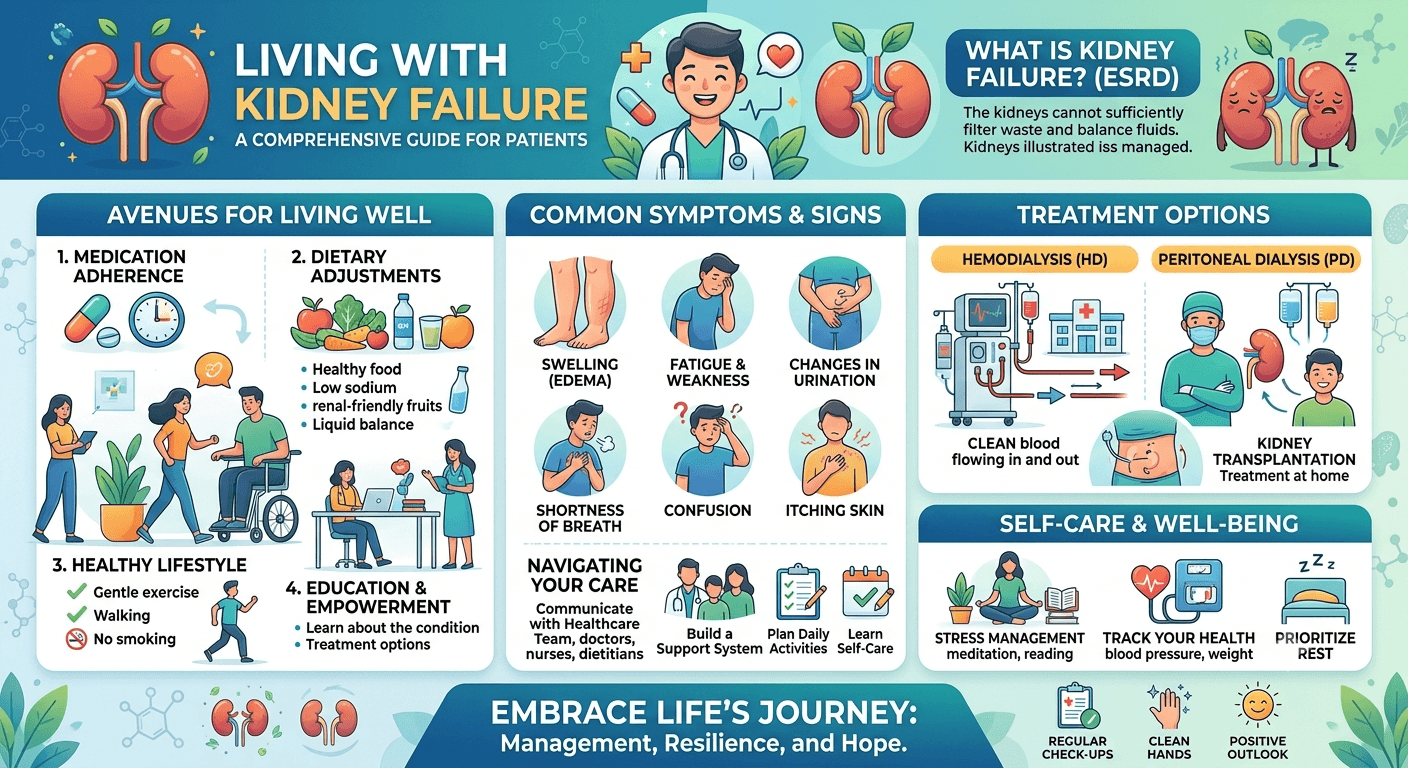
Dialysis
When kidney function declines to the point where waste products and excess fluid can no longer be adequately removed, dialysis becomes necessary.
There are two main types:
- Hemodialysis: Blood is filtered through a dialysis machine, usually three times per week at a dialysis center or, in some cases, at home.
- Peritoneal Dialysis: The lining of the abdomen (peritoneum) acts as a natural filter. Dialysis fluid is infused into and drained from the abdominal cavity, allowing waste removal at home.
Dialysis is a life-sustaining treatment but does not cure kidney failure.
Kidney Transplantation
For eligible patients with end-stage kidney disease, a kidney transplant offers the best long-term outcomes. A healthy kidney from a living or deceased donor is surgically implanted, restoring many normal kidney functions.
After transplantation, lifelong immunosuppressive medications are required to prevent organ rejection.
Medications Used in Kidney Failure
Medication regimens are tailored to each patient’s needs and may include:
- ACE inhibitors or ARBs: Help control blood pressure and reduce protein loss in the urine.
- Diuretics: Help remove excess fluid and reduce swelling.
- Sodium-glucose cotransporter-2 (SGLT2) inhibitors: In selected patients with diabetes or chronic kidney disease, these medications can slow kidney disease progression and reduce cardiovascular risk.
- Phosphate binders: Lower phosphorus levels in the blood.
- Vitamin D analogs: Support bone health and calcium balance.
- Erythropoiesis-stimulating agents (ESAs): Treat anemia associated with chronic kidney disease.
- Iron supplements: Correct iron deficiency and support red blood cell production.
- Potassium-lowering medications: Used when high potassium levels pose a risk.
Summary
Kidney failure is a serious condition that develops when the kidneys can no longer effectively remove waste products, excess fluid, and toxins from the blood. It may occur suddenly as acute kidney injury (AKI) or progress gradually as chronic kidney disease (CKD). Early recognition of symptoms, timely diagnosis, and appropriate treatment can slow disease progression, prevent complications, and improve quality of life.
Read More https://kdigo.org