Diabetic ketoacidosis (DKA) is a severe and potentially fatal complication of diabetes caused by a lack of insulin along with increased levels of counter-regulatory hormones such as glucagon, cortisol, catecholamines, and growth hormone. These hormonal imbalances result in high blood glucose levels, ketone formation, and metabolic acidosis.
Pathophysiology
DKA is an acute metabolic emergency most commonly associated with type 1 diabetes, although it may also develop in individuals with type 2 diabetes during periods of significant stress or illness. It occurs due to either absolute or relative insulin deficiency combined with elevated counter-regulatory hormones.
Mechanism
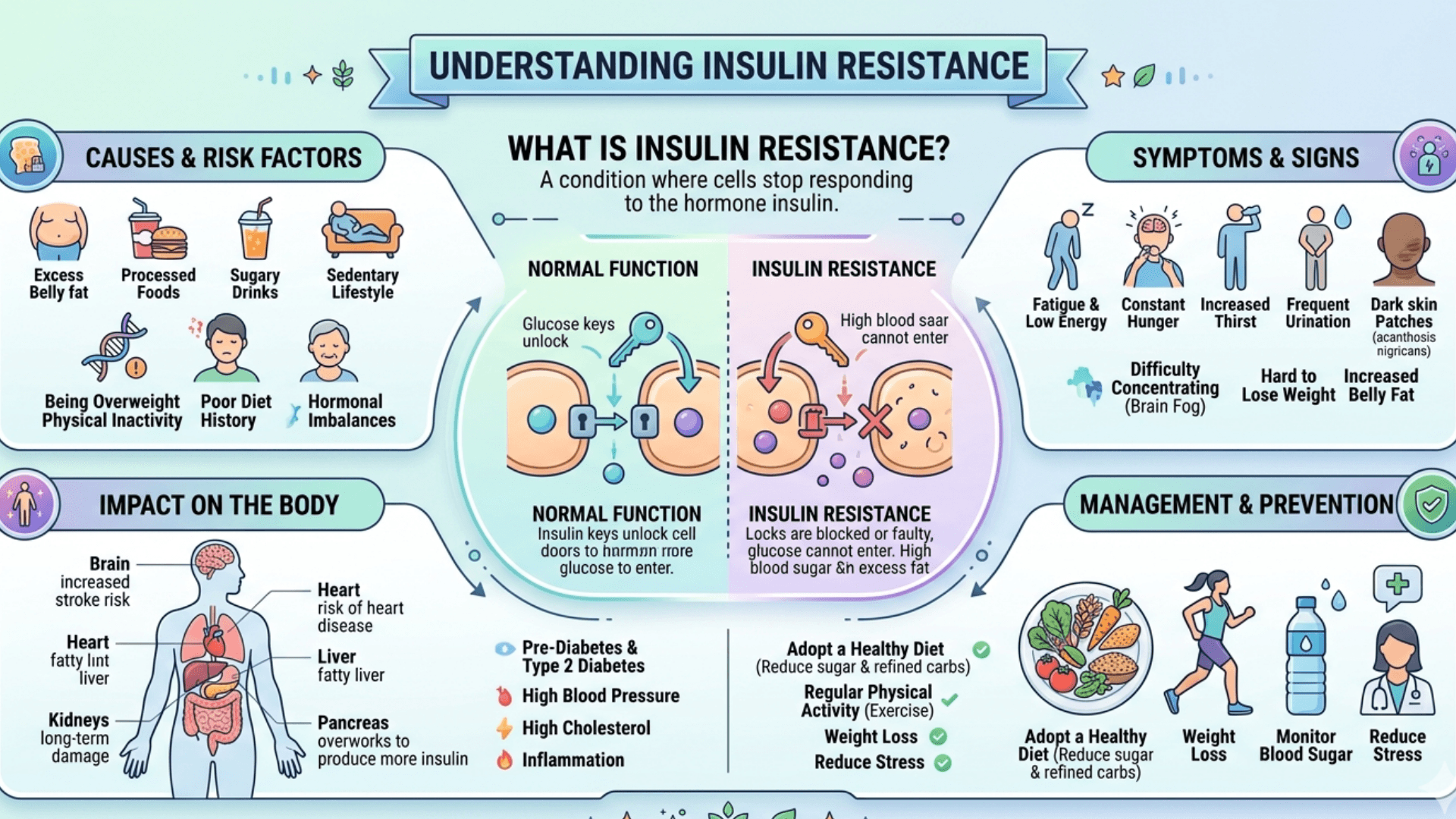
- Inadequate insulin prevents glucose from entering muscle and fat cells while simultaneously stimulating glucose production in the liver through gluconeogenesis and glycogen breakdown, leading to marked hyperglycemia.
- Reduced insulin and elevated stress hormones trigger lipolysis, releasing free fatty acids into the bloodstream.
- The liver converts these fatty acids into ketone bodies, including acetoacetate, β-hydroxybutyrate, and acetone, through ketogenesis.
- Excess ketone accumulation causes metabolic acidosis.
- Elevated glucose levels produce osmotic diuresis, resulting in dehydration, electrolyte depletion particularly potassium loss and impaired kidney perfusion, all of which aggravate acidosis and hyperglycemia.
The defining features of DKA are hyperglycemia, ketosis, and metabolic acidosis. Metabolic Dysfunction.
Causes
DKA commonly develops when factors either increase insulin requirements or reduce insulin availability. Major causes include:
Poor Insulin Management
- Missing insulin injections or insulin pump failure.
- Insufficient adjustment of insulin during illness or stressful conditions.
b. Infections
- The leading precipitating factor for DKA.
- Frequently associated infections include pneumonia, urinary tract infections, and sepsis.
- Inflammatory responses during infection increase stress hormones and worsen insulin resistance.
c. Newly Diagnosed Diabetes.
- DKA may be the first indication of previously undiagnosed type 1 diabetes.
d. Other Triggers.
- Acute medical conditions such as myocardial infarction, stroke, or pancreatitis.
- Emotional or physical stress.
- Medications including corticosteroids, thiazide diuretics, sympathomimetics, and SGLT2 inhibitors.
Clinical Manifestations
symptoms of Diabetic ketoacidosis (DKA)
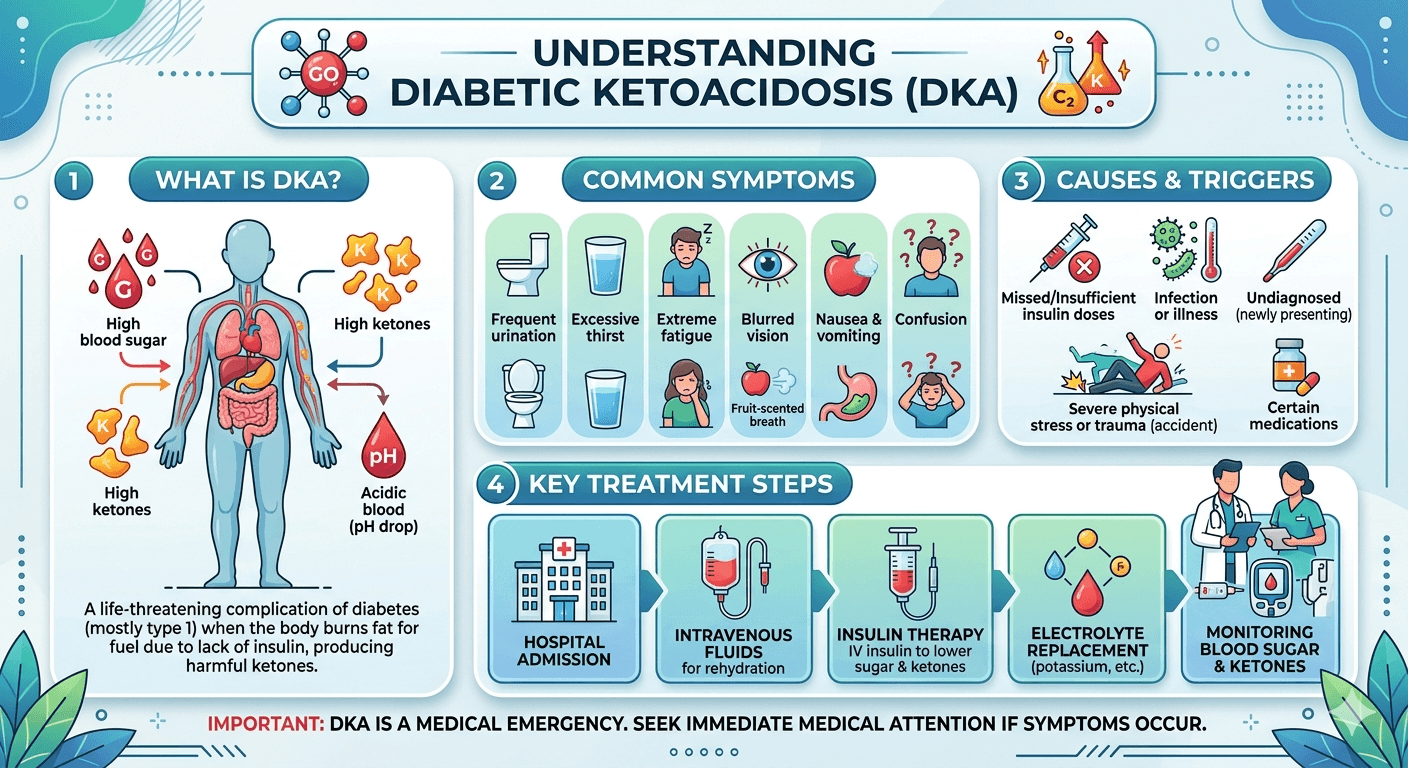
Diabetic ketoacidosis (DKA) is a serious and potentially life-threatening complication of diabetes that occurs when the body lacks sufficient insulin and begins breaking down fat for energy, leading to the accumulation of acidic ketone bodies in the blood.
Common symptoms of DKA include:
- Excessive thirst (polydipsia) and frequent urination (polyuria) due to high blood glucose levels.
- Dry mouth and signs of dehydration.
- Nausea, vomiting, and abdominal pain, which may be severe.
- Fatigue, weakness, and lethargy.
- Unexplained weight loss over a short period.
- Rapid, deep breathing (Kussmaul respiration) as the body attempts to correct acidosis.
- Fruity or acetone-like breath odor caused by ketone production.
- Blurred vision.
- Confusion, drowsiness, or altered mental status, especially in severe cases.
- In advanced DKA, loss of consciousness or coma may occur.
DKA requires urgent medical attention. Early recognition and prompt treatment with fluids, insulin, and electrolyte replacement are essential to prevent serious complications and death.
Advanced Symptoms
- Nausea and vomiting due to ketosis and acidosis.
- Abdominal pain, especially common in children.
- Fruity-smelling breath caused by acetone exhalation.
- Kussmaul respirations, characterized by deep and labored breathing as compensation for metabolic acidosis.
Signs of dehydration such as dry mucous membranes, reduced skin turgor, hypotension, and tachycardia
Neurological Changes
Altered consciousness ranging from confusion to coma in severe cases.
Management
Successful treatment of DKA requires immediate correction of metabolic disturbances and identification of the underlying trigger.
Initial Evaluation
Diagnosis is confirmed through laboratory findings such as:
- Blood glucose greater than 250 mg/dL.
- Arterial pH below 7.3.
- Serum bicarbonate less than 18 mEq/L.
- Presence of ketones in blood or urine.
Healthcare providers should also assess hydration status, mental state, vital signs, and possible precipitating factors.
Fluid Replacement
- Treatment begins with intravenous 0.9% normal saline at 15–20 mL/kg during the first hour.
- Further fluid therapy depends on hemodynamic status, sodium levels, and urine output.
- When glucose levels fall below 200 mg/dL, dextrose-containing fluids are added to prevent hypoglycemia while insulin therapy continues.
Insulin Administration
- Continuous regular insulin infusion at 0.1 units/kg/hour is started after initial fluid replacement.
- Initial insulin boluses are generally avoided to reduce the risk of rapid osmotic shifts.
- Insulin therapy continues until acidosis resolves and the anion gap normalizes.
Electrolyte Correction
- Potassium replacement is essential:
- If potassium is below 3.3 mEq/L, insulin should be delayed until potassium is corrected.
- If potassium is between 3.3 and 5.0 mEq/L, potassium is added to IV fluids.
- If potassium exceeds 5.0 mEq/L, supplementation is withheld but closely monitored.
- Bicarbonate therapy is usually reserved for severe acidosis with pH below 6.9.
Ongoing Monitoring
- Hourly glucose monitoring.
- Frequent checks of electrolytes, venous pH, and anion gap every 2–4 hours.
- Continuous cardiac monitoring to detect arrhythmias related to potassium imbalance.
Treating the Underlying Cause
Any precipitating condition such as infection, medication-related issues, or stress must be identified and appropriately managed.
Transition to Subcutaneous Insulin
After DKA resolves and oral intake resumes, IV insulin should overlap with subcutaneous insulin administration for 1–2 hours to prevent rebound hyperglycemia.
Prevention and Education
Patients should receive education on:
- Adherence to insulin therapy.
- Sick-day management.
- Monitoring blood glucose and ketones.
- Recognizing early warning signs and seeking timely medical care.
General Dietary Guidelines
Foods to Include
- Complex carbohydrates: whole grains, oats, brown rice, sweet potatoes
- Lean proteins: chicken, fish, eggs, tofu, legumes
- Healthy fats: avocado, olive oil, nuts, seeds
- High-fiber vegetables: spinach, broccoli, cucumber, carrots
- Low-sugar fruits: berries, apples, pears
- Plenty of water and electrolyte-rich fluids
Foods to Avoid
- Sugary drinks and desserts
- Refined carbohydrates (white bread, pastries)
- Fried and processed foods
- Excess salt and saturated fats
- Alcohol and energy drinks
Conclusion
DKA is a medical emergency characterized by hyperglycemia, ketosis, and metabolic acidosis resulting from insulin deficiency and elevated stress hormones. Common triggers include infection, missed insulin therapy, acute illness, and certain medications. Early recognition and prompt treatment with IV fluids, insulin, electrolyte correction, and management of the underlying cause are essential for recovery. With proper diabetes management, patient education, and adherence to treatment, DKA is largely preventable. Proper nutrition, along with insulin adherence and glucose monitoring, plays an important role in preventing recurrent diabetic ketoacidosis and maintaining stable blood sugar levels.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional regarding any medical condition or health-related concerns. The author and publisher are not responsible for any actions taken based on the information presented in this article.