Causes, Complications, and Management
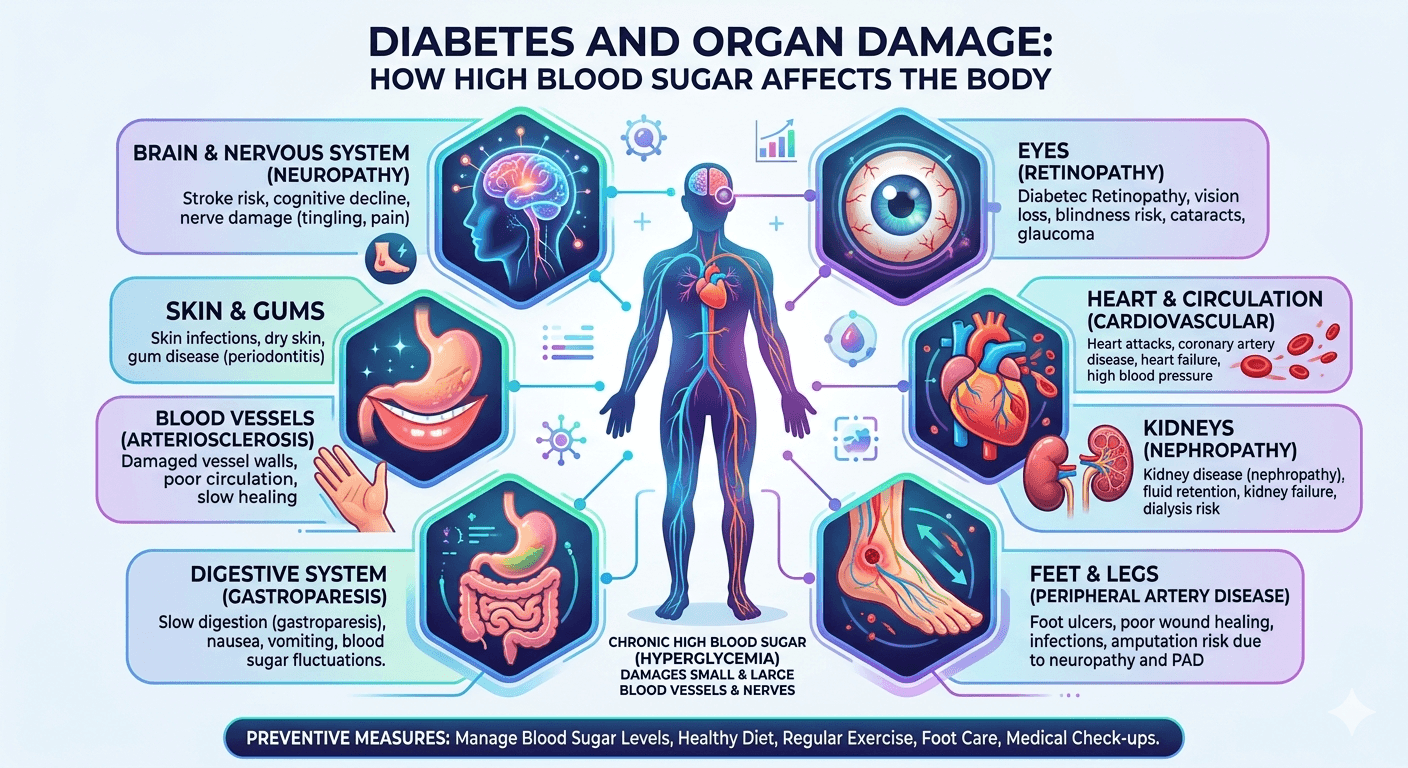
Diabetes mellitus is a long-term metabolic disease that affects far more than blood sugar levels. The relationship between Diabetes and organ damage is a major health concern, as chronic hyperglycemia can gradually harm multiple body systems. Over time, elevated glucose levels damage blood vessels, impair nerve function, and promote inflammation and oxidative stress. These changes contribute to the development of both microvascular and macrovascular complications, affecting organs such as the kidneys, eyes, heart, and nervous system. Understanding these underlying mechanisms and adopting effective preventive measures are crucial for reducing complications, improving quality of life, and lowering the risk of premature death in individuals with diabetes.
Diabetes can silently damage vital organs, including the kidneys, heart, eyes, nerves, and liver. Learn how high blood sugar leads to long-term complications, recognize early warning signs, and discover effective strategies to prevent organ damage and maintain overall health.
Pathophysiology of Organ Damage
The principal mechanism underlying diabetic complications is sustained hyperglycemia, which exerts harmful effects in several ways:
Vascular Dysfunction
Microvascular injury: Affects small blood vessels, particularly in the retina, kidneys, and peripheral nerves.
Macrovascular injury: Involves large arteries, increasing risk of coronary artery disease, cerebrovascular disease, and peripheral arterial disease.
Neuropathy
Hyperglycemia impairs nerve blood supply and function, resulting in sensory, motor, and autonomic deficits.
Inflammation and Oxidative Stress
Excess glucose promotes free radical formation and low-grade inflammation, accelerating cellular and tissue injury.
Major Complications of Diabetes
https://www.youtube.com/watch?v=oJnrQIwlwDI
Diabetic ketoacidosis (DKA)
Diabetic ketoacidosis (DKA) is a severe and potentially fatal complication of diabetes caused by a lack of insulin along with increased levels of counter-regulatory hormones such as glucagon, cortisol, catecholamines, and growth hormone. These hormonal imbalances result in high blood glucose levels, ketone formation, and metabolic acidosis.
Diabetic Retinopathy
Ophthalmic (Diabetic Retinopathy): Microvascular leakage and vessel proliferation may cause visual impairment or blindness.
Types:
Non-Proliferative Diabetic Retinopathy (NPDR):
- Early stage.
- Features: microaneurysms, dot/blot hemorrhages, hard exudates, macular edema.
Proliferative Diabetic Retinopathy (PDR):
- Advanced stage.
- Features: neovascularization, vitreous hemorrhage, tractional retinal detachment.
Symptoms:
- Often asymptomatic in early stages.
- Blurred or fluctuating vision.
- Dark spots (floaters).
- Vision loss in advanced disease.
Renal (Diabetic Nephropathy)
Diabetic nephropathy is one of the most common and serious complications of diabetes. It occurs when persistently high blood sugar levels damage the tiny blood vessels (glomeruli) in the kidneys, reducing their ability to filter waste and excess fluid from the blood. Early stages may not cause noticeable symptoms, but progressive kidney damage can lead to protein leakage in the urine, swelling of the legs, high blood pressure, and eventually chronic kidney disease or kidney failure.
Regular monitoring of blood glucose, blood pressure, kidney function tests, and urine protein levels is essential for early detection and management. Maintaining good diabetes control can significantly reduce the risk of diabetic nephropathy and other kidney and urinary disorders associated with long-term diabetes.
Progressive glomerular damage can lead to proteinuria, chronic kidney disease, and end-stage renal failure.
Key Features:
- Early sign: Microalbuminuria (small amounts of protein in urine).
- Progression: Can advance to proteinuria, reduced kidney function, and eventually chronic kidney disease (CKD) or end-stage renal disease (ESRD).
- Symptoms: Often silent in the early stages; later may include swelling of feet/ankles, fatigue, high blood pressure, and foamy urine.
- Risk factors: Poorly controlled blood sugar, long duration of diabetes, hypertension, smoking, and genetic predisposition.
Cardiovascular
Increased risk of myocardial infarction, heart failure, hypertension, and atherosclerosis.
Key Effects:
- Atherosclerosis: Faster buildup of fatty plaques in arteries, causing narrowing and stiffness.
- Coronary Artery Disease (CAD): Higher risk of angina, heart attacks, and ischemic heart disease.
- Hypertension: Common in diabetics, further straining the heart and vessels.
- Cardiomyopathy: Structural and functional changes in the heart muscle, leading to heart failure.
- Peripheral Artery Disease (PAD): Reduced blood flow to limbs, causing pain, ulcers, and risk of gangrene.
- Stroke: Increased likelihood of cerebrovascular accidents due to vascular damage and clot formation.
Neurological (Peripheral and Autonomic Neuropathy)
Manifestations include pain, numbness, gastrointestinal dysmotility, and erectile dysfunction.
Peripheral Neuropathy
- Neuropathy
- Affects nerves in the hands, feet, and legs.
- Symptoms: Numbness, tingling, burning or stabbing pain, reduced ability to feel temperature or touch.
- Complications: Increased risk of foot ulcers, infections, and amputations due to unnoticed injuries.
Autonomic Neuropathy
Involves nerves controlling involuntary body functions.
Possible effects:
- Heart: Resting tachycardia, silent heart attacks, abnormal blood pressure regulation.
- Digestive system: Gastroparesis, constipation, or diarrhea.
- Urinary system: Bladder dysfunction, urinary retention or incontinence.
- Sexual function: Erectile dysfunction in men, vaginal dryness in women.
- Sweating and temperature control abnormalities.
Foot Complications
Neuropathy and ischemia predispose to ulcers, infections, and amputations.
Dermatological and Oral Health Issues
Higher susceptibility to infections, periodontal disease, and delayed wound healing.
Neurological (Central Nervous System)
Elevated risk of cognitive decline, vascular dementia, and Alzheimer’s disease.
Management and Preventive Strategies
Early intervention and sustained management are critical to mitigating complications.
Glycemic Control
- Self-monitoring of blood glucose and HbA1c testing.
- Adherence to pharmacological treatment (oral hypoglycemics, insulin, or combination therapy).
- Dietary modifications emphasizing low glycemic index foods, fiber, lean protein, and limited refined carbohydrates.
Cardiovascular Risk Management
- Blood pressure target: <130/80 mmHg.
- Lipid control with statins when indicated.
- Sodium restriction and avoidance of processed foods.
Lifestyle Modifications
- At least 150 minutes of moderate-intensity physical activity per week.
- Weight reduction in overweight/obese individuals.
- Smoking cessation and moderation of alcohol intake.
Routine Monitoring and Screening
- Annual dilated eye examination.
- Regular urine albumin-to-creatinine ratio and serum creatinine testing for nephropathy.
- Comprehensive foot examination for neuropathy and ulcer prevention.
- Cardiovascular assessment based on risk profile.
Psychosocial and Behavioral Interventions
- Stress management to reduce cortisol-mediated glucose fluctuations.
- Sleep hygiene to support metabolic stability.
Conclusion
Diabetes is a multisystem disease with the potential to cause severe organ damage if inadequately controlled. The burden of complications such as retinopathy, nephropathy, cardiovascular disease, and neuropathy underscores the importance of comprehensive care. Through tight glycemic control, cardiovascular risk reduction, lifestyle interventions, and regular screening, the progression of diabetic complications can be significantly delayed or prevented.
Effective diabetes management today is the foundation for long-term organ protection and improved patient outcomes.