Viral hepatitis refers to inflammation of the liver caused by specific viruses that target liver cells. The main culprits are hepatitis A, B, C, D, and E viruses. These infections vary in how they spread, how long they last, and how severely they affect the liver.
Pathophysiology
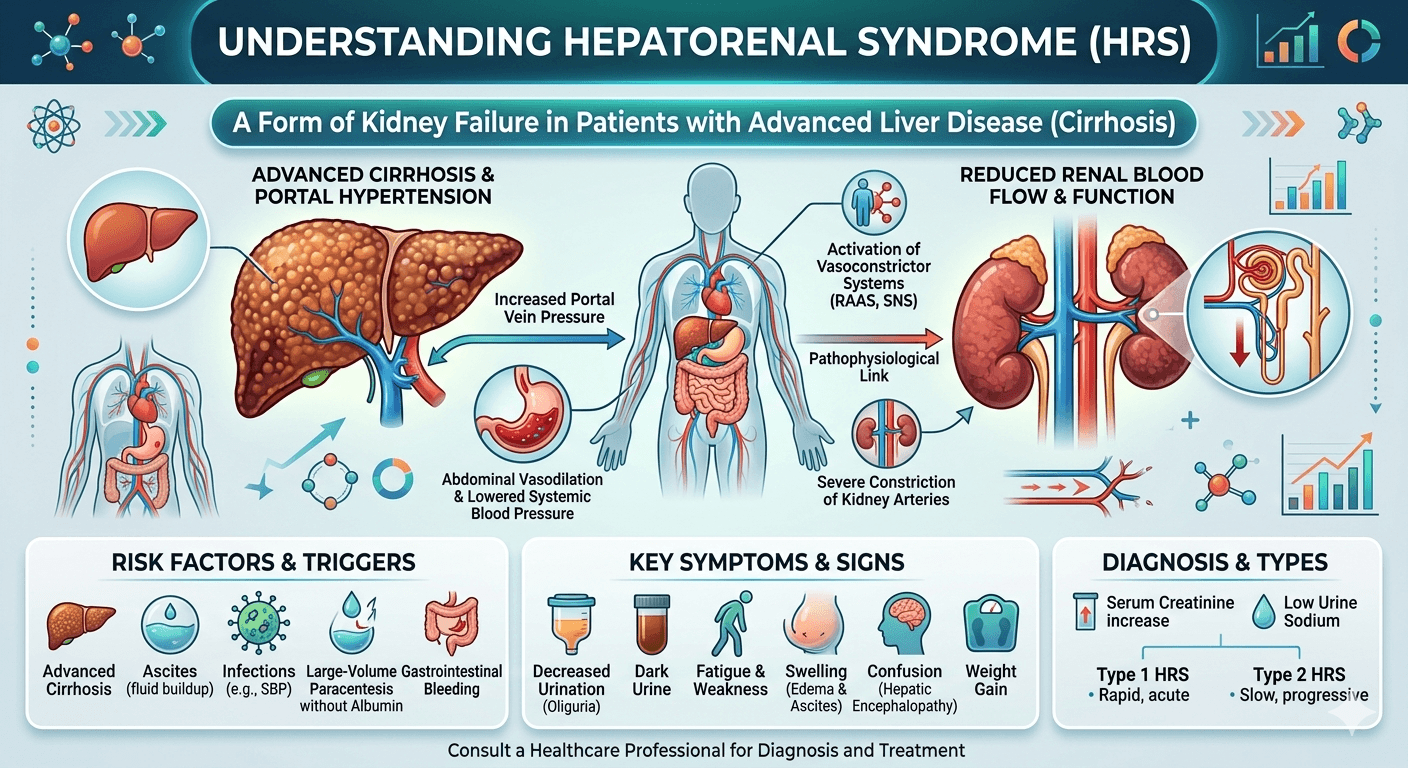
The liver damage in viral hepatitis results from two main processes: the direct impact of the virus on liver cells and the body’s immune response to infection.
- Inside the liver cells:
The viruses enter hepatocytes and replicate using the cell’s machinery. Some, like hepatitis B, can integrate parts of their genetic material into the host’s DNA, allowing them to persist for years. Others, such as hepatitis A and E, are cleared after a short infection. Viral replication can interfere with normal cell functions like protein synthesis and metabolism. - Immune response:
The immune system detects infected liver cells and attacks them. Cytotoxic T cells and inflammatory cytokines cause cell death and inflammation, leading to elevated liver enzymes and jaundice. When the immune attack continues over time, it triggers fibrosis, cirrhosis, and can eventually lead to liver cancer. - Potential complications:
These include acute liver failure from massive cell death, chronic hepatitis that progresses to cirrhosis, and hepatocellular carcinoma. Coinfection (for example, HBV with HDV) or a weakened immune system can make the disease more severe.
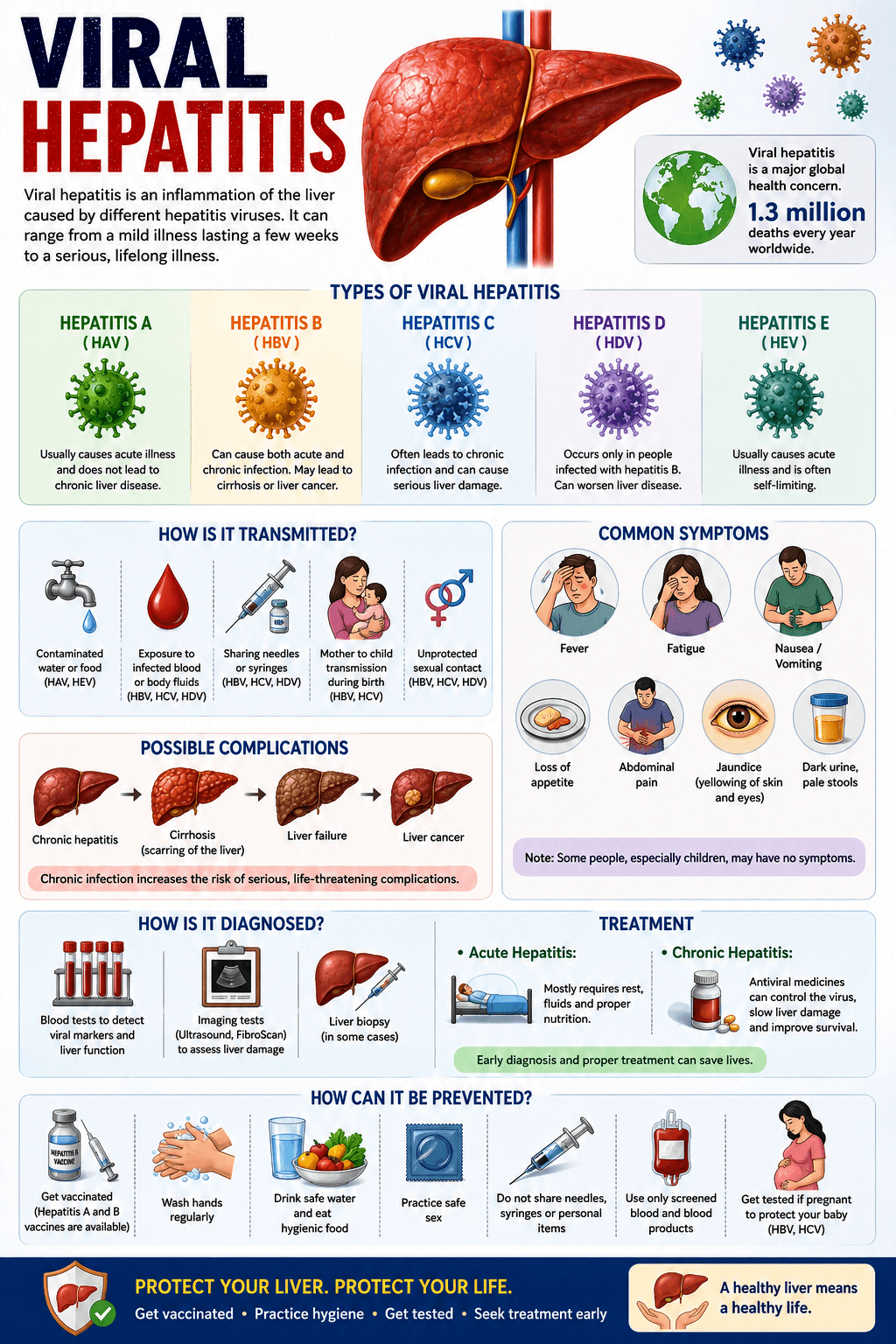
Types of Viral Hepatitis
Hepatitis A (HAV)
- Type: RNA virus (Picornavirus).
- Transmission: Fecal–oral route via contaminated food, water, or contact with infected individuals.
- Course: Usually an acute, short-term illness. Rarely causes severe liver failure. No chronic infection. An effective vaccine is available.
Hepatitis B (HBV)
- Type: DNA virus (Hepadnavirus).
- Transmission: Blood and body fluids (birth, sex, needles, transfusions).
- Course: May be acute or chronic. Infants infected at birth have a higher risk of developing chronic disease. Chronic HBV can lead to cirrhosis and liver cancer. A highly effective vaccine and antiviral treatments (tenofovir, entecavir) are available.
Hepatitis C (HCV)
- Type: RNA virus (Flavivirus).
- Transmission: Primarily through blood exposure (needles, transfusions before screening, unsafe medical practices).
- Course: Often becomes chronic and can slowly cause fibrosis, cirrhosis, and liver cancer. Modern antiviral drugs (DAAs) cure over 95% of cases. No vaccine yet.
Hepatitis D (HDV)
- Type: Defective RNA virus that requires HBV to replicate.
- Transmission: Same as HBV.
- Course: Occurs as a Coinfection with HBV or as a super infection in HBV carriers. Super infection tends to cause more severe disease. Prevention relies on HBV vaccination.
Hepatitis E (HEV)
- Type: RNA virus (Hepevirus).
- Transmission: Fecal–oral, often through contaminated water; can also spread from animals.
- Course: Usually acute and self-limited but can be severe in pregnant women. Chronic HEV may occur in immunocompromised individuals. A vaccine exists in some countries but is not widely used.
Causes and Risk Factors
Viral hepatitis is mainly caused by infection with hepatitis viruses such as Hepatitis A, Hepatitis B, Hepatitis C, Hepatitis D, and Hepatitis E. These viruses attack the liver and cause inflammation, which can lead to liver damage if not treated properly.
Several risk factors increase the chance of developing viral hepatitis. These include poor hygiene, unsafe drinking water, blood transfusions without proper screening, intravenous drug use, multiple sexual partners, healthcare exposure to infected blood, tattooing or piercing with unsterilized equipment, and weakened immunity. Lack of vaccination, especially for hepatitis A and B, also increases the risk of infection.
Clinical Features
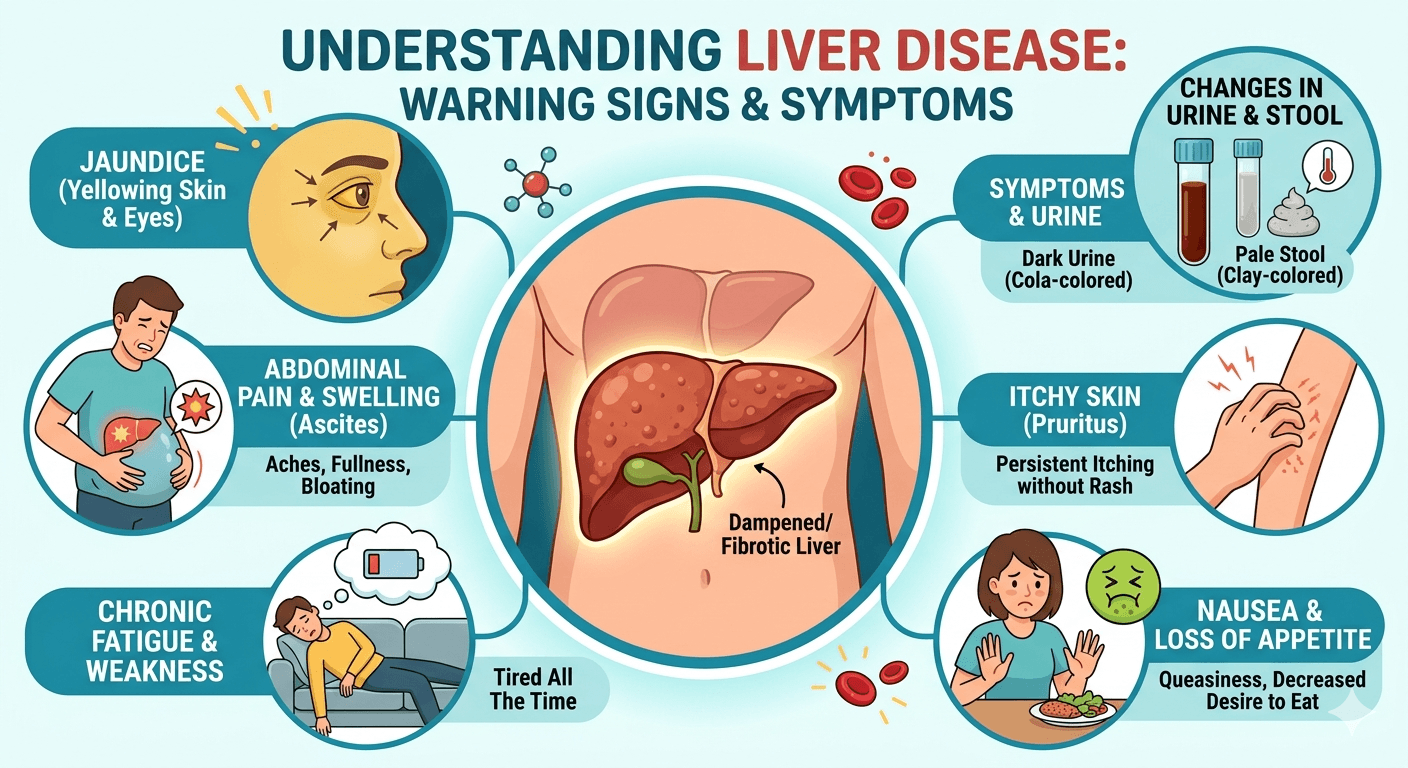
The symptoms of viral hepatitis may vary from mild illness to serious liver complications. During the initial stage, patients often report tiredness, weakness, fever, reduced appetite, nausea, vomiting, body aches, and pain or discomfort in the upper right side of the abdomen. As the condition advances, jaundice can appear, leading to yellowing of the skin and eyes, dark urine, and pale-colored stools.
Certain individuals may also develop itching, liver enlargement, and mild pain in the joints. In chronic infections, particularly Hepatitis B and Hepatitis C, symptoms can remain unnoticed for many years before progressing to complications such as liver fibrosis, cirrhosis, or liver failure. Advanced disease may cause mental confusion, increased bleeding tendency, and abdominal swelling as a result of severe liver damage.
Line of Management
Prevention:
- Vaccines: Available for HAV and HBV (which also prevents HDV). Universal infant HBV vaccination is key to prevention.
- Public health measures: Safe food and water, blood screening, sterile injections, safe sex, and harm reduction programs for people who inject drugs.
- Expanding vaccination and treatment access supports WHO’s global elimination goals.
Diagnosis and Screening:
- HAV: IgM anti-HAV confirms acute infection.
- HBV: HBsAg, anti-HBs, and HBV DNA for diagnosis and monitoring.
- HCV: Anti-HCV for screening; HCV RNA to confirm active infection.
- HDV: Test in HBsAg-positive individuals using anti-HDV or HDV RNA.
- HEV: IgM anti-HEV or HEV RNA testing for acute cases.
Screening recommendations vary, but many countries now advocate one-time HBV and HCV testing for adults.
Treatment
- HAV and HEV: Supportive care only; rest, hydration, and avoiding alcohol or liver-toxic drugs.
- HBV: Long-term antivirals (tenofovir, entecavir) to control viral replication and prevent progression to cirrhosis or liver cancer.
- HCV: Short courses of oral DAAs that cure most infections. Common oral DAAs include sofosbuvir, ledipasvir, daclatasvir, velpatasvir, and glecaprevir/pibrentasvir. Treatment choice depends on the HCV genotype, liver condition, and patient-related factors.
- HDV: Difficult to treat; pegylated interferon and newer therapies are under study. HBV vaccination remains the best prevention.
Lifestyle and follow-up
Avoid alcohol, manage metabolic conditions, and ensure vaccination of household contacts. Long-term follow-up includes liver enzyme testing, fibrosis assessment, and cancer screening (ultrasound, and AFP every six months for cirrhotic patients).
Patient education
Education should include the importance of completing prescribed treatment, attending regular follow-up visits, and monitoring liver function. Patients should avoid alcohol, smoking, and unnecessary medications that may further damage the liver. A balanced diet, adequate rest, and healthy lifestyle habits can help support liver recovery.
Family members and close contacts may also require screening or vaccination to reduce transmission. Proper counseling helps improve treatment adherence, reduce stigma, and enhance the overall quality of life of patients with viral hepatitis.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional regarding any medical condition or health-related concerns. The author and publisher are not responsible for any actions taken based on the information presented in this article.