Causes, Pathophysiology, and Management
Definition and Overview
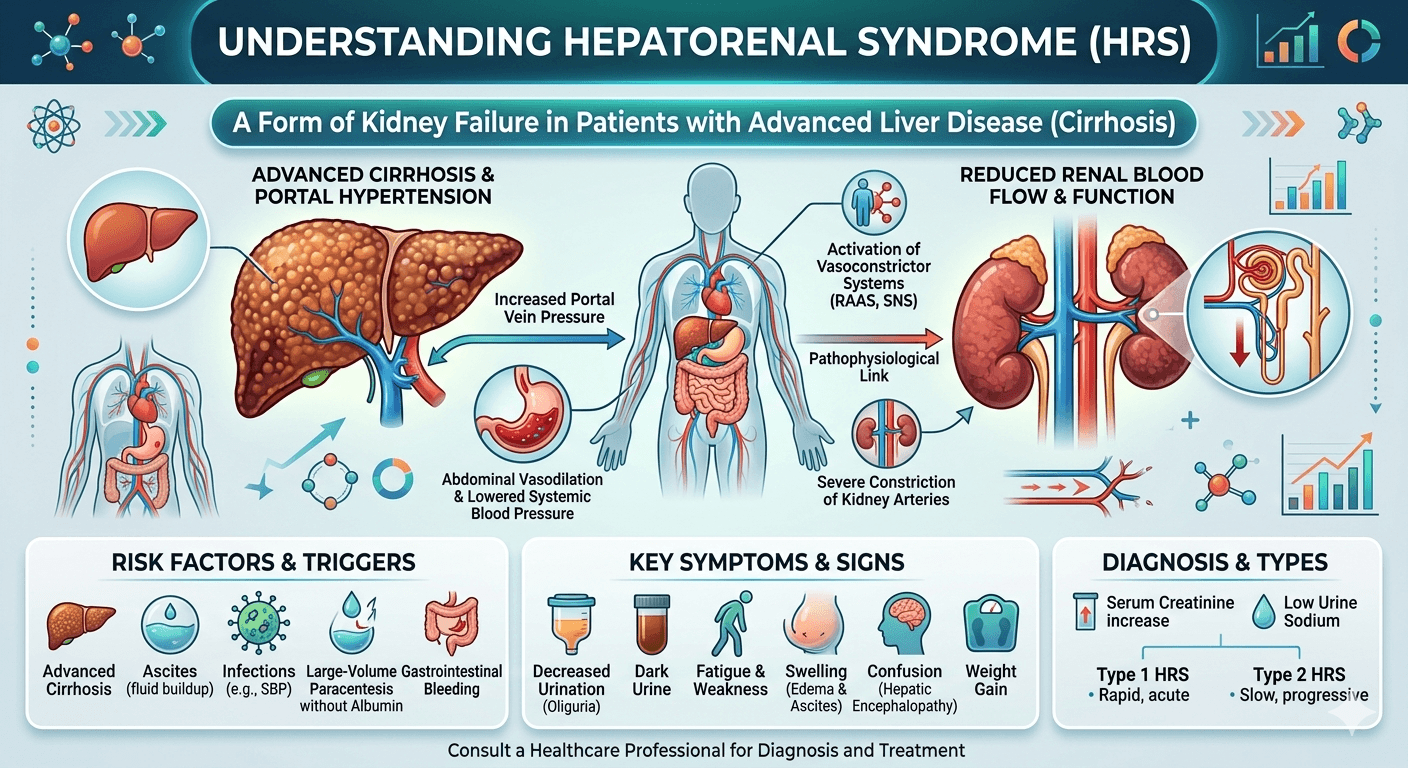
Hepatorenal syndrome is defined as the development of renal failure in individuals with severe liver disease, most often cirrhosis, in the absence of any identifiable cause of kidney dysfunction. The syndrome results from alterations in blood flow and vascular regulation, leading to intense constriction of blood vessels in the kidneys and failure of the renal filtration process. HRS typically occurs in the context of worsening liver function, often triggered by infections, gastrointestinal bleeding, or excessive use of diuretics.
Pathophysiology
The main mechanism underlying HRS is an imbalance between vasodilation and vasoconstriction, resulting in reduced blood flow to the kidneys.
- Splanchnic Vasodilation
Portal hypertension in liver disease triggers the release of vasodilators such as nitric oxide.
This widens blood vessels in the Splanchnic circulation (gut and abdominal organs), lowering effective blood volume.
Activation of Vasoconstrictor Systems
To compensate, the body activates the RAAS (rennin–angiotensin–aldosterone system), sympathetic nervous system, and antidiuretic hormone.
These responses cause sodium and water retention, Ascites, and progressive renal vasoconstriction.
- Systemic Inflammation
Bacterial translocation from the gut and endotoxin release aggravate vascular dysfunction and accelerate renal impairment.
Causes and Risk Factors
HRS does not develop spontaneously but is usually precipitated by specific events in patients with advanced cirrhosis or acute liver failure.
Primary liver conditions:
- Decompensated cirrhosis (most common) is the stage of chronic liver disease where the liver can no longer perform its essential functions adequately, and serious complications begin to appear.
- Severe alcoholic hepatitis
- Acute fulminant hepatic failure
Precipitating factors:
- Spontaneous bacterial peritonitis (SBP)
- Large-volume paracentesis without albumin replacement
- Gastrointestinal bleeding
- Overuse of diuretics leading to hypovolemia.
- Severe infections or sepsis
Types of Hepatorenal Syndrome
Hepatorenal syndrome (HRS) is a severe complication of advanced liver disease in which kidney function deteriorates quickly even though the kidneys remain structurally intact. It most often develops in individuals with decompensated cirrhosis and significant portal hypertension.
Type 1 Hepatorenal Syndrome (HRS-AKI)
This is the rapidly worsening form of HRS. Kidney failure appears over a period of days to weeks and is marked by a significant increase in serum creatinine levels. Common triggers include infections such as spontaneous bacterial peritonitis, gastrointestinal hemorrhage, or profound dehydration. Patients may experience decreased urine output, increasing ascites, confusion, and marked fatigue. Type 1 HRS has a poor outlook and demands immediate management with vasoconstrictor medications, albumin administration, and consideration of liver transplantation.
Type 2 Hepatorenal Syndrome
This form is more gradual and chronic in nature. Kidney impairment develops slowly and is frequently linked with refractory Ascites that responds poorly to diuretic treatment. Early symptoms are usually milder, although the disorder may worsen progressively. Treatment focuses on managing Ascites, providing albumin therapy, and assessing suitability for liver transplantation.
Updated Classification
Current guidelines divide HRS into:
- HRS-AKI (Acute Kidney Injury) → equivalent to the previous Type 1 HRS
- HRS-NAKI (Non-Acute Kidney Injury) → includes chronic or subacute kidney impairment, similar to the former Type 2 HRS
Prompt recognition and treatment are essential because Hepatorenal syndrome is linked to high mortality in patients with advanced liver disease.
HRS Type 1: Rapidly progressive, with doubling of serum creatinine (>2.5 mg/dL) or halving of creatinine clearance within 2 weeks. Poor prognosis, median survival ~2 weeks if untreated.
HRS Type 2: More slowly progressive, commonly associated with refractory Ascites. Median survival ~6 months.
Diagnosis
HRS is a diagnosis of exclusion, made after ruling out structural kidney injury or other causes of renal dysfunction. Key criteria include:
- Advanced liver disease with portal hypertension and Ascites
- Low GFR (elevated serum creatinine or low urine output)
- No shock, nephrotoxic drug use, or structural kidney disease
- Lack of improvement after diuretic withdrawal and plasma volume expansion with albumin
Lab Tests
- CBC
- LFT (Liver function test)
- KFT (kidney function test) with electrolytes.
- Lipid Profile
- RBS with HBA1C
- Urinalysis
Imaging
- USG (whole abdomen)
- CT Scan or MRI (whole abdomen)
Management
1. General Principles
- Remove or correct precipitating factors (infections, bleeding, over-diuresis).
- Discontinue nephrotoxic drugs (NSAIDs, Aminoglycosides, contrast agents).
- Avoid hypovolemia and correct electrolyte imbalances.
2. Pharmacological Therapy
Vasoconstrictors + Albumin are the mainstay:
Terlipressin + Albumin (gold standard where available).
Alternatives: Norepinephrine, Midodrine + Octreotide + Albumin (especially where Terlipressin is not available).
Albumin: Expands plasma volume and counteracts circulatory dysfunction.
3. Supportive Measures
- Careful fluid balance.
- Treat infections aggressively (antibiotics, albumin infusion for SBP).
- Avoid further renal insults.
4. Renal Replacement Therapy
- Dialysis may be required as a bridge to liver transplantation.
- Not a definitive therapy but supports patients with severe renal dysfunction.
5. Definitive Treatment
- Liver Transplantation: The only curative treatment, as it corrects the underlying liver failure and restores renal function in most cases.
- Simultaneous liver–kidney transplantation may be considered in selected patients with prolonged renal dysfunction.
Prognosis
- Untreated HRS has extremely poor survival (weeks to months).
- Early recognition and initiation of vasoconstrictor therapy with albumin improve short-term outcomes.
- Liver transplantation remains the only intervention that significantly improves long-term survival.
Conclusion
Hepatorenal syndrome is a severe complication of advanced liver disease, characterized by functional renal failure due to systemic and Splanchnic circulatory disturbances. Prompt recognition, correction of precipitating factors, vasoconstrictor plus albumin therapy, and timely referral for liver transplantation are critical for improving patient outcomes.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional regarding any medical condition or health-related concerns. The author and publisher are not responsible for any actions taken based on the information presented in this article.
Read more about diabetes and organ damage