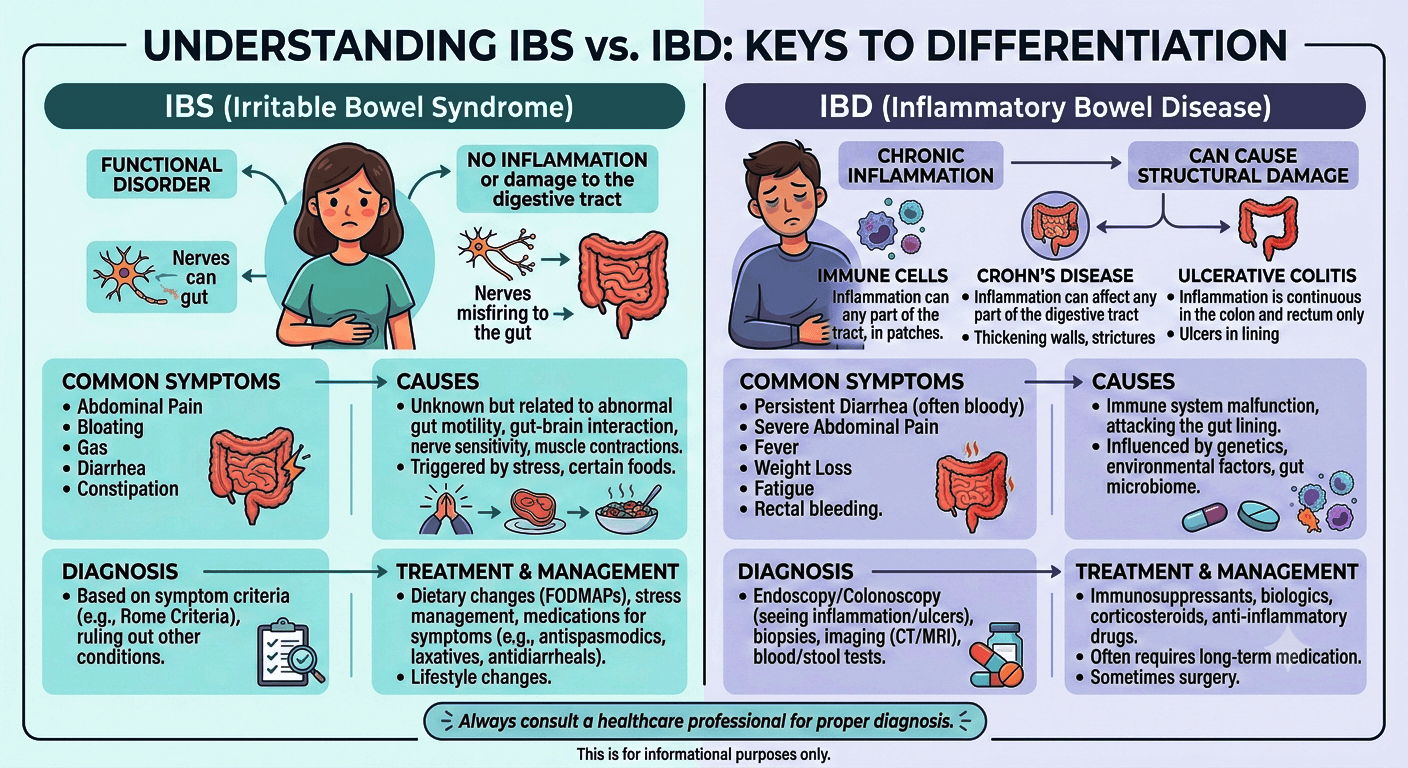
IBS vs. IBD: What Is the Difference?
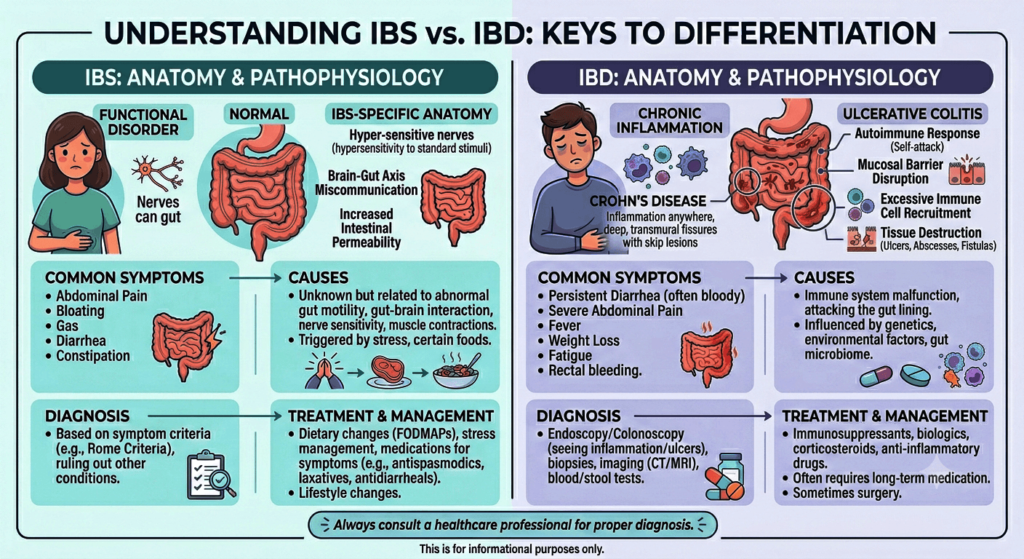
IBS (Irritable Bowel Syndrome) is a functional disorder causing chronic abdominal pain, bloating, and altered bowel habits, but no structural damage. IBD (Inflammatory Bowel Disease), including Crohn’s and ulcerative colitis, is a serious autoimmune condition causing chronic inflammation, tissue ulcers, and visible damage to the digestive tract.
Introduction
Digestive disorders affect millions of people worldwide, but many people are confused by the terms IBS and IBD. Although their names sound similar and both can cause symptoms such as abdominal pain, diarrhea, and changes in bowel habits, they are fundamentally different conditions. Irritable Bowel Syndrome (IBS) is a functional gastrointestinal disorder that impacts how the digestive tract works without causing visible inflammation or permanent damage. Inflammatory Bowel Disease (IBD), on the other hand, is a group of chronic inflammatory conditions that cause ongoing inflammation and structural damage to the gastrointestinal tract.
Understanding the difference between IBS vs. IBD is important because their causes, diagnostic approaches, treatments, and long-term health implications vary significantly. While IBS can greatly impact quality of life, IBD may lead to serious complications if left untreated. This guide explores the key differences between IBS and IBD, including their symptoms, causes, diagnosis, treatment options, and when to seek medical attention.
Understanding IBS and IBD
What Is IBS?
Irritable Bowel Syndrome (IBS) is a functional gastrointestinal disorder. This means that the digestive tract appears structurally normal but does not function properly.
In IBS:
- The intestines are not damaged.
- No significant inflammation is present.
- Symptoms arise from abnormal gut motility, altered gut-brain communication, and increased intestinal sensitivity.
IBS affects millions of people worldwide and is one of the most common reasons for gastroenterology consultations.
Common Types of IBS
- IBS-D: Predominantly diarrhea
- IBS-C: Predominantly constipation
- IBS-M: Mixed diarrhea and constipation
- IBS-U: Unclassified
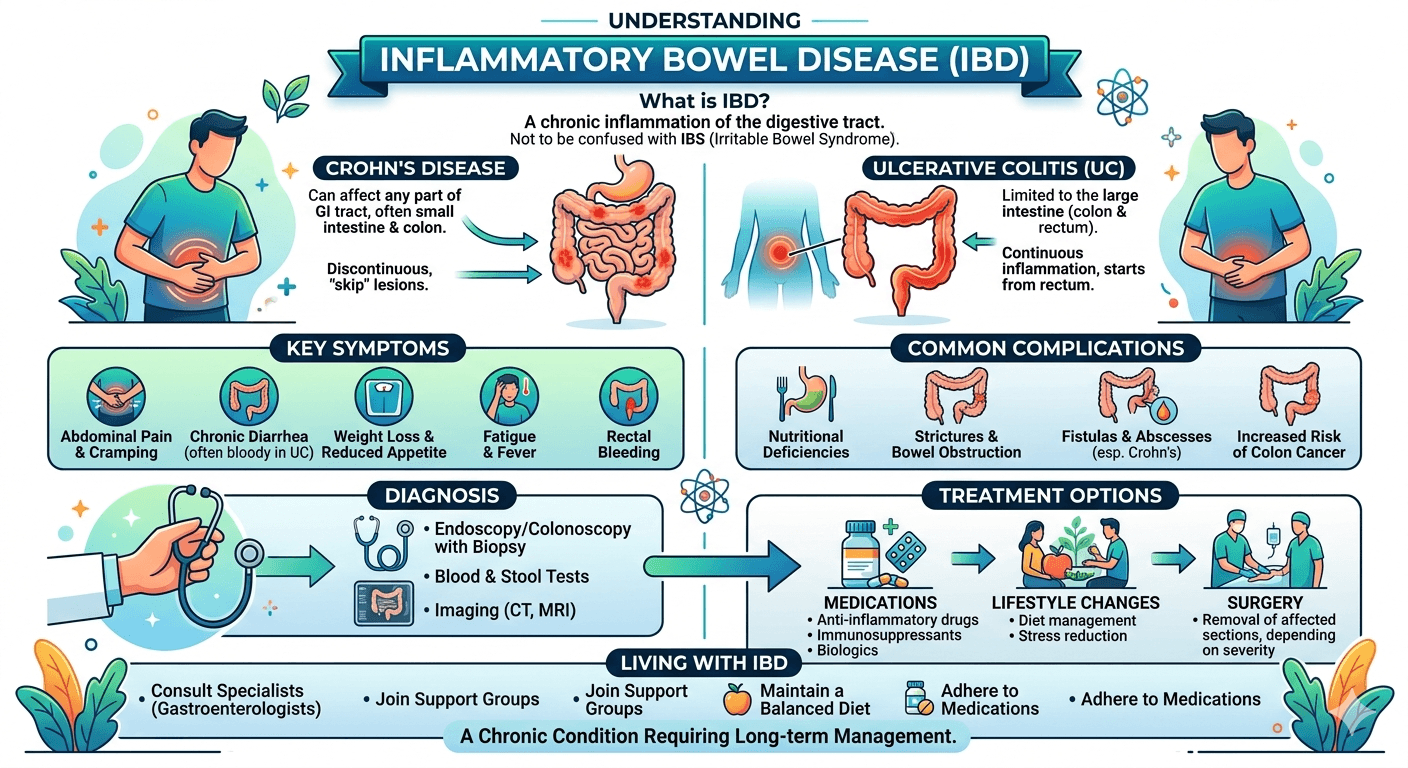
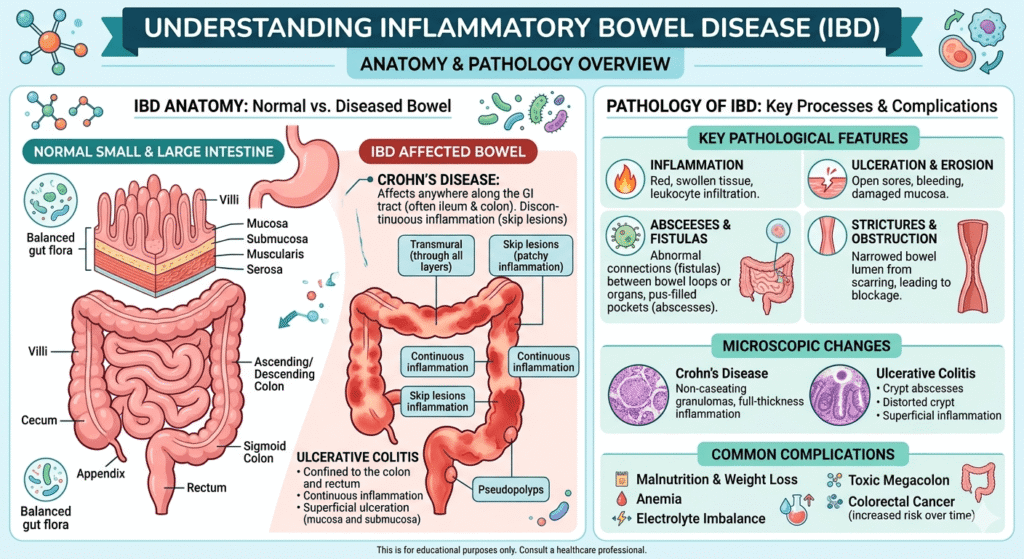
What Is IBD?
Inflammatory Bowel Disease (IBD) is a group of chronic inflammatory disorders that cause actual damage to the digestive tract.
The two major forms are:
Crohn’s Disease
Can impact any part of the gastrointestinal tract, from the mouth to the anus.
Characteristics:
- Patchy areas of inflammation (“skip lesions”)
- Involves the entire bowel wall thickness
- May cause fistulas and strictures
Ulcerative Colitis
Affects only the colon and rectum.
Characteristics:
- Continuous inflammation
- Limited primarily to the inner lining of the colon
- Often causes bloody diarrhea (Gastrointestinal bleeding)
Unlike IBS, IBD causes visible inflammation and tissue injury.
IBS vs. IBD: Key Differences at a Glance
| Feature | IBS | IBD |
| Type of Condition | Functional disorder | Inflammatory disease |
| Intestinal Damage | No | Yes |
| Inflammation | Minimal or absent | Significant |
| Bleeding | Rare | Common |
| Cancer Risk | No increased risk | Increased risk in some patients |
| Weight Loss | Uncommon | Common |
| Fever | Rare | May occur |
| Blood Tests | Usually normal | Often abnormal |
| Colonoscopy Findings | Typically normal | Inflammation visible |
| Life-Threatening Complications | Rare | Possible |
Causes of IBS
The exact cause of IBS remains incompletely understood.
Most experts believe multiple factors contribute.
Common Causes and Risk Factors
Gut-Brain Axis Dysfunction
The gut and brain communicate continuously.
In IBS:
- Signals become exaggerated.
- The brain can interpret the normal, everyday movements of the gut as painful sensations.
Abnormal Intestinal Motility
Food may move:
- Too quickly (diarrhea)
- Too slowly (constipation)
Visceral Hypersensitivity
Visceral hypersensitivity is an increased sensitivity to sensations arising from internal organs, especially the gastrointestinal (GI) tract. People with visceral hypersensitivity may experience pain, discomfort, bloating, or urgency from normal levels of intestinal stretching or activity that would not bother most people.
Stress and Psychological Factors
Stress does not cause IBS directly but often worsens symptoms.
Common associations include:
- Anxiety
- Depression
- Chronic stress
Microbiome Changes
Alterations in gut bacteria may contribute to symptoms.
Less Common Contributing Factors
- Prior gastrointestinal infections
- Food intolerances
- Small intestinal bacterial overgrowth (SIBO)
- Genetic predisposition
Causes of IBD
Unlike IBS, IBD involves a true inflammatory process.
Immune System Dysfunction
The immune system mistakenly attacks the digestive tract.
This leads to:
- Chronic inflammation
- Tissue injury
- Ulcer formation
Genetic Factors
Numerous genetic variants increase susceptibility.
Having a close relative with IBD significantly raises risk.
Environmental Factors
Potential triggers include:
- Smoking (especially Crohn’s disease)
- Western dietary patterns
- Certain infections
- Urban living environments
Microbiome Alterations
Changes in intestinal bacteria may activate abnormal immune responses.
Symptoms of IBS
IBS symptoms typically fluctuate over time.
Many patients describe periods of improvement followed by flare-ups.
Typical Symptoms
Abdominal Pain
A hallmark symptom.
Pain often:
- Improves after bowel movements
- Varies in intensity
- Recurs frequently
Bloating
Patients frequently describe:
- Abdominal fullness
- Distension
- Excess gas
Diarrhea
Particularly in IBS-D.
May include:
- Urgency
- Frequent loose stools
Constipation
Common in IBS-C.
May involve:
- Hard stools
- Straining
- Incomplete evacuation
Mixed Bowel Habits
Alternating constipation and diarrhea.
Symptoms Not Typical of IBS
The presence of these symptoms should prompt further evaluation:
- Blood in stool
- Fever
- Significant weight loss
- Nighttime symptoms
- Persistent anemia
Symptoms of IBD
IBD symptoms are often more severe and progressive.
Digestive Symptoms
Chronic Diarrhea
May occur multiple times daily.
Blood in Stool
Particularly common in ulcerative colitis.
Abdominal Pain
Usually caused by active inflammation.
Urgent Bowel Movements
Patients may struggle to delay defecation.
Systemic Symptoms
Because IBD is an inflammatory disease, symptoms may affect the whole body.
Fatigue
One of the most common complaints.
Weight Loss
Results from:
- Poor absorption
- Reduced appetite
- Chronic inflammation
Fever
May occur during active disease.
Extraintestinal Manifestations
IBD can impact organs beyond the gut.
Examples include:
- Arthritis
- Eye inflammation
- Skin disorders
- Liver disease
For medical students, these extraintestinal manifestations are important diagnostic clues.
How IBS and IBD Are Diagnosed
Diagnosis begins with a thorough clinical evaluation.
Medical History
Doctors assess:
- Symptom patterns
- Duration
- Family history
- Dietary triggers
- Associated symptoms
Physical Examination
May reveal:
- Abdominal tenderness
- Signs of malnutrition
- Weight loss
- Dehydration
IBS examinations are often normal.
IBD may show objective abnormalities.
Blood Tests
Common tests include:
- Complete Blood Count (CBC)
- C-reactive Protein (CRP)
- Erythrocyte Sedimentation Rate (ESR)
- Electrolytes
- Liver function tests
- Lipid profile
- RBS & HbA1c
Findings
IBS:
- Usually normal
- RBS & HbA1c (abnormal finding if patient is diabetic)
IBD:
May show:
- Elevated inflammatory markers
- Anemia
- Nutritional deficiencies
Stool Tests
Doctors may test for:
- Infection
- Blood
- Fecal calprotectin
Elevated fecal calprotectin strongly suggests intestinal inflammation and helps distinguish IBD from IBS.
Endoscopy and Colonoscopy
These are among the most essential investigations for IBD.
Doctors can:
- Visualize inflammation
- Obtain biopsies
- Assess disease severity
IBS typically shows normal findings.
Imaging Studies
Ultrasound
Can evaluate:
- Bowel wall thickness
- Abscesses
- Inflammation
CT Scan
Useful for:
- Complications
- Acute flare-ups
- Abscess detection
MRI
Particularly valuable for:
- Crohn’s disease
- Fistulas
- Pelvic involvement
Biopsy
Tissue samples obtained during colonoscopy confirm the diagnosis.
Potential Complications of IBS
IBS does not damage the intestines, but it can significantly impact quality of life.
Complications include:
- Chronic discomfort
- Anxiety
- Depression
- Social limitations
- Work and school absenteeism
Importantly, IBS does not increase the risk of colon cancer.
Potential Complications of IBD
IBD can lead to serious complications.
Intestinal Complications
Crohn’s Disease
- Fistulas
- Abscesses
- Strictures
- Bowel obstruction
Ulcerative Colitis
- Severe bleeding
- Toxic megacolon
- Colon perforation
Nutritional Problems
Patients may develop:
- Iron deficiency
- Vitamin B12 deficiency
- Protein malnutrition
Cancer Risk
Long-standing IBD increases the risk of colorectal cancer, especially when inflammation is extensive and poorly controlled.
Treatment of IBS
Treatment focuses on symptom management.
Dietary Changes
Many patients benefit from:
- Low-FODMAP diets
- Increased fiber (selected patients)
- Identifying trigger foods
Common triggers include:
- Caffeine
- Alcohol
- Fatty foods
Stress Management
Helpful strategies include:
- Cognitive behavioral therapy
- Meditation
- Regular exercise
- Mindfulness techniques
Medications
Depending on symptoms:
- Anti diarrheals
- Laxatives
- Antispasmodics
- Certain antidepressants
Treatment of IBD
Treatment aims to control inflammation and prevent complications.
Anti-Inflammatory Medications
Examples:
- Mesalamine
- Sulfasalazine
Corticosteroids
Used for short-term flare control.
Examples:
- Prednisone
- Budesonide
Immunomodulators
Help suppress abnormal immune activity.
Examples:
- Azathioprine
- Methotrexate
Biologic Therapies
Modern treatments targeting specific inflammatory pathways.
Examples:
- Anti-TNF agents
- Integrin inhibitors
- IL-12/23 inhibitors
Surgery
It may be necessary for:
- Severe disease
- Obstruction
- Fistulas
- Cancer prevention
Surgery can cure ulcerative colitis by removing the colon but does not cure Crohn’s disease.
Living With IBS and IBD
Receiving a diagnosis can feel overwhelming. Fortunately, both conditions can be managed effectively.
Practical Lifestyle Advice
Keep a Symptom Diary
Track:
- Foods
- Stress levels
- Medications
- Symptoms
Patterns often emerge.
Follow Medical Advice
Regular follow-up improves outcomes.
Stay Physically Active
Exercise can:
- Improve bowel function
- Reduce stress
- Support overall health
Prioritize Mental Health
Digestive disorders and emotional health are closely linked.
Seeking support is a sign of strength, not weakness.
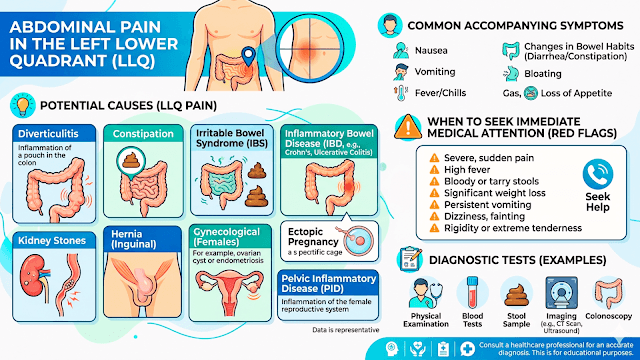
When to Seek Medical Attention
Contact a healthcare professional if you experience:
- Blood in stool
- Persistent weight loss
- Fever
- Severe abdominal pain
- Nighttime diarrhea
- Symptoms that worsen despite treatment
These may indicate IBD or another serious condition rather than IBS.
Final Thoughts
The differentiation between IBS and IBD remains the most crucial topic in gastroenterology. Although similar in many ways as far as symptoms and severity are concerned, there exist several differences that make each of the diseases biologically unique.
On the patient’s side, learning about the difference between the two disorders will help decrease anxiety levels and get proper medical attention. For a medical student, on the other hand, such differentiation becomes key in assessing the problem.
Most importantly, whether it is IBS or IBD that a person has, adequate management and good relations with his/her healthcare provider can truly change one’s life.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment.