Pelvic Inflammatory Disease (PID) often develops silently, making it easy to overlook its earliest symptoms. Recognizing the early warning signs of Pelvic Inflammatory Disease, such as mild pelvic discomfort, unusual vaginal discharge, or pain during intercourse, is essential for timely diagnosis. Because untreated PID can lead to serious complications, including infertility, understanding these early warning signs of Pelvic Inflammatory Disease can help you seek prompt medical care and prevent long-term reproductive health problems.
Introduction
As a medical professional, one of the most concerning aspects of PID is that its early symptoms can be subtle. Many women dismiss the initial signs as menstrual discomfort, digestive issues, or a mild urinary infection. Unfortunately, delayed treatment can lead to serious complications, including chronic pelvic pain, infertility, ectopic pregnancy, and recurrent infections.
Recognizing the early warning signs is therefore crucial. This article explores the 10 early warning signs of Pelvic Inflammatory Disease (PID) you should never ignore, providing practical insights for patients and foundational knowledge for medical students.
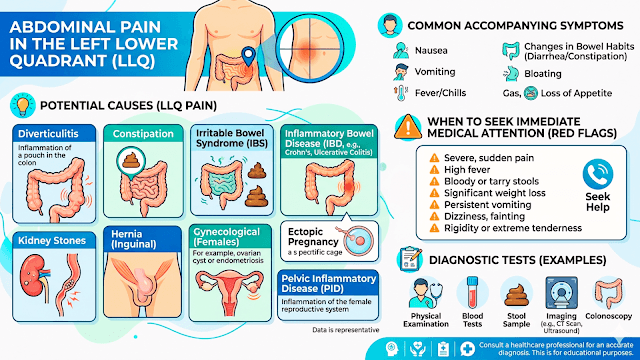
What Is Pelvic Inflammatory Disease (PID)?
PID refers to inflammation and infection involving the upper female genital tract, including:
- The uterus (endometrium)
- Fallopian tubes (salpingitis)
- Ovaries
- Surrounding pelvic tissues
The infection usually begins in the lower reproductive tract and gradually spreads upward. The inflammatory response can cause tissue damage, scarring, and adhesions that may permanently affect reproductive health.
Common Risk Factors
Risk factors include:
- Multiple sexual partners
- Unprotected sexual intercourse
- Previous history of PID
- Previous STI infection
- Recent insertion of an intrauterine device (IUD)
- Douching
- Age younger than 25 years with active sexual activity
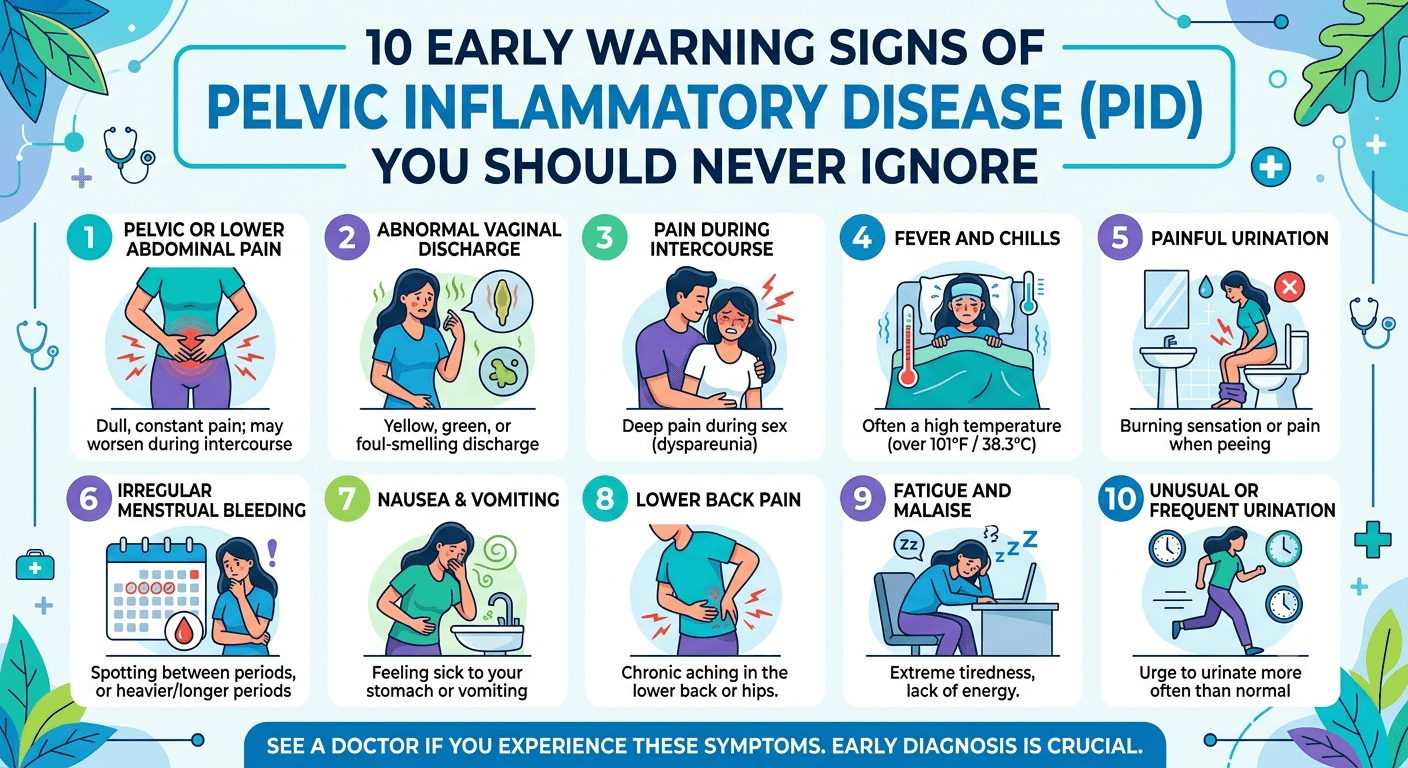
10 Early Warning Signs of Pelvic Inflammatory Disease (PID) You Should Never Ignore
1. Persistent Lower Abdominal or Pelvic Pain
The most common early symptom of PID is pain in the lower abdomen or pelvis.
Why It Happens
As bacteria spread into the upper reproductive organs, inflammation develops. This inflammatory process irritates surrounding tissues and nerves, resulting in discomfort or pain.
Typical Characteristics
- Dull, aching pain
- Mild to moderate intensity initially
- May affect one or both sides of the pelvis
- Often worsens over time
Many patients mistake this symptom for menstrual cramps, delaying medical evaluation.
Medical Student Note
Pelvic pain is considered a hallmark symptom of PID and is part of the minimal clinical criteria often used for diagnosis.
2. Unusual Vaginal Discharge
Changes in vaginal discharge frequently appear early in the disease process.
What to Look For
Discharge may become:
- Yellow or green
- Thick or purulent
- Foul-smelling
- Excessively abundant
Clinical Significance
The abnormal discharge reflects infection in the cervix and reproductive tract. Patients often report noticing a change in odor or consistency before other symptoms become obvious.
Differential Diagnosis
Medical students should remember that abnormal discharge may also occur in:
- Bacterial vaginosis
- Yeast infections
- Cervicitis
- Certain STIs
The presence of pelvic pain alongside discharge increases suspicion for PID.
3. Pain During Sexual Intercourse
Painful intercourse, medically known as dyspareunia, is another early warning sign.
Mechanism
Inflamed reproductive organs become sensitive to pressure and movement during sexual activity.
Patient Experience
Women may describe:
- Deep pelvic pain during intercourse
- Pain that persists afterward
- Progressive worsening over weeks
This symptom should never be dismissed as a normal variation in sexual experience.
4. Irregular Menstrual Bleeding
Abnormal uterine bleeding can occur early in PID and PCOS.
Possible Manifestations
- Spotting between periods
- Heavier-than-normal periods
- Bleeding after intercourse
- Unexpected bleeding patterns
Underlying Cause
Inflammation affects the lining of the uterus and cervix, disrupting normal bleeding patterns.
Clinical Importance
Any new menstrual irregularity accompanied by pelvic discomfort warrants medical assessment.
5. Painful Urination
Many women with early PID experience discomfort while urinating.
Symptoms Include
- Burning sensation
- Increased urgency
- Frequent urination
- Mild pelvic pressure
Why It Can Be Misleading
Patients often assume they have a urinary tract infection (UTI). While UTIs are common, persistent urinary symptoms combined with pelvic pain should raise suspicion for PID.
Urinary symptoms in PID may occur due to inflammation of adjacent pelvic structures (cystitis) rather than direct urinary tract infection.
6. Low-Grade Fever
A mild fever is a sign that the body’s immune system is responding to infection.
Typical Presentation
- Temperature between 37.8°C and 38.5°C (100°F–101.3°F)
- Accompanied by malaise
- May fluctuate throughout the day
Why It Matters
Even a low-grade fever should not be ignored when occurring with pelvic symptoms.
Clinical Relevance
Fever is considered an additional supportive criterion for PID diagnosis.
7. Fatigue and General Malaise
Many infectious diseases cause systemic symptoms, and PID is no exception.
Common Complaints
Patients frequently report:
- Feeling unusually tired
- Lack of energy
- Reduced concentration
- Generalized weakness
Pathophysiology
Inflammatory cytokines released during infection contribute to fatigue and a sense of illness.
Because fatigue is nonspecific, it is often overlooked despite being an important clue.
8. Nausea and Digestive Discomfort
As inflammation progresses, gastrointestinal symptoms may emerge.
Possible Symptoms
- Nausea
- Loss of appetite
- Mild abdominal bloating
- Occasional vomiting
Diagnostic Challenge
PID may mimic:
- Gastroenteritis
- Appendicitis
- Irritable bowel syndrome
- Ovarian disorders
For this reason, clinicians should always consider reproductive tract pathology in women presenting with abdominal complaints.
9. Lower Back Pain
Pelvic infections frequently produce referred pain.
Characteristics
- Dull ache in the lower back
- Persistent discomfort
- Associated pelvic symptoms
Why It Occurs
Inflammation within the pelvis can irritate nerves that also supply structures in the lower back.
Clinical Pearl
Lower back pain alone is rarely diagnostic, but in combination with vaginal discharge and pelvic pain, it becomes more significant.
10. Cervical Motion Tenderness
This is a key clinical sign identified during a pelvic examination.
What Is It?
When a healthcare provider gently moves the cervix during examination, the patient experiences significant pain.
Why It Happens
Inflamed reproductive organs become extremely sensitive, and movement transmits pressure throughout the infected tissues.
Cervical motion tenderness is one of the classic findings associated with PID and is often remembered as part of the diagnostic triad:
- Cervical motion tenderness
- Uterine tenderness
- Adnexal tenderness
Although patients may not recognize this sign themselves, it remains an important early indicator identified by clinicians.
Potential Complications of Untreated PID
Ignoring early symptoms can have serious consequences.
Infertility
Repeated inflammation may scar the fallopian tubes, preventing fertilization.
Ectopic Pregnancy
Tubal damage increases the risk of implantation outside the uterus, most commonly within a fallopian tube.
Chronic Pelvic Pain
Persistent inflammation and scarring can lead to long-term pain that significantly affects quality of life.
Tubo-Ovarian Abscess
Severe infections may form abscesses requiring hospitalization or surgery.
Recurrent PID
A previous episode increases susceptibility to future infections.
How PID Is Diagnosed
Diagnosis often combines:
Clinical Assessment
Healthcare providers evaluate:
- Symptoms
- Sexual history
- Risk factors
- Pelvic examination findings
Laboratory Testing
Tests may include:
- STI screening (HIV, Hepatitis B & C, VDRL)
- Cervical swabs
- Pregnancy testing
- Blood tests for inflammation(ESR,CRP)
- Kidney function test (KFT)
- Urine Test
Imaging
Pelvic ultrasound may help identify:
- Tubo-ovarian abscesses
- Fluid collections
- Alternative diagnoses
- TVS (transvaginal ultrasound)
Treatment of PID
Early treatment is essential.
Antibiotics
Most patients receive broad-spectrum antibiotics that target likely bacterial causes.
Vaginal pessary tablets
Treatment often begins before laboratory confirmation because delaying therapy increases the risk of complications.
Partner Treatment
Sexual partners may also require evaluation and treatment to prevent reinfection.
Follow-Up Care
Patients should:
- Complete the full antibiotic course
- Attend follow-up appointments
- Avoid sexual activity until treatment is completed
Frequently Asked Questions (FAQs)
Can PID occur without an STI?
Yes. Although STIs are common causes, PID can also result from other bacteria that naturally inhabit the vagina.
Can PID go away on its own?
No. Untreated PID can progress and cause permanent reproductive damage. Medical treatment is necessary.
Is PID always painful?
Not always. Some women experience mild or even silent infections, which is why routine screening is important.
Can PID cause infertility?
Yes. Scarring of the fallopian tubes can interfere with conception and increase the risk of infertility.
How quickly does PID develop?
The progression varies. Symptoms may appear gradually over days to weeks following infection.
Can PID return after treatment?
Yes. Reinfection can occur, especially if sexual partners are not treated or if new infections develop.
Is hospitalization always required?
No. Many cases are treated successfully with outpatient antibiotics, although severe infections may require hospitalization.
Can PID affect pregnancy?
Previous PID increases the risk of infertility and ectopic pregnancy. Active infection during pregnancy requires immediate medical evaluation.
Conclusion
Pelvic inflammatory disease is a very serious problem that usually starts with mild symptoms. These are the 10 first symptoms of Pelvic Inflammatory Disease (PID) which you should pay attention to: pain in pelvis, vaginal discharge, pain during sexual intercourse, irregular menstruation, pain when urinating, fever, tiredness, nausea, pain in the lower back and pain on examination of cervix. Timely identification of these symptoms allows preventing serious problems such as infertility, chronic pelvic pain and ectopic pregnancy.
It is important for patients to understand these symptoms as a way to prevent reproductive problems. For medical students who need to learn about this problem, these symptoms will be an excellent background for identification and management of PID.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional regarding any medical condition or health-related concerns.