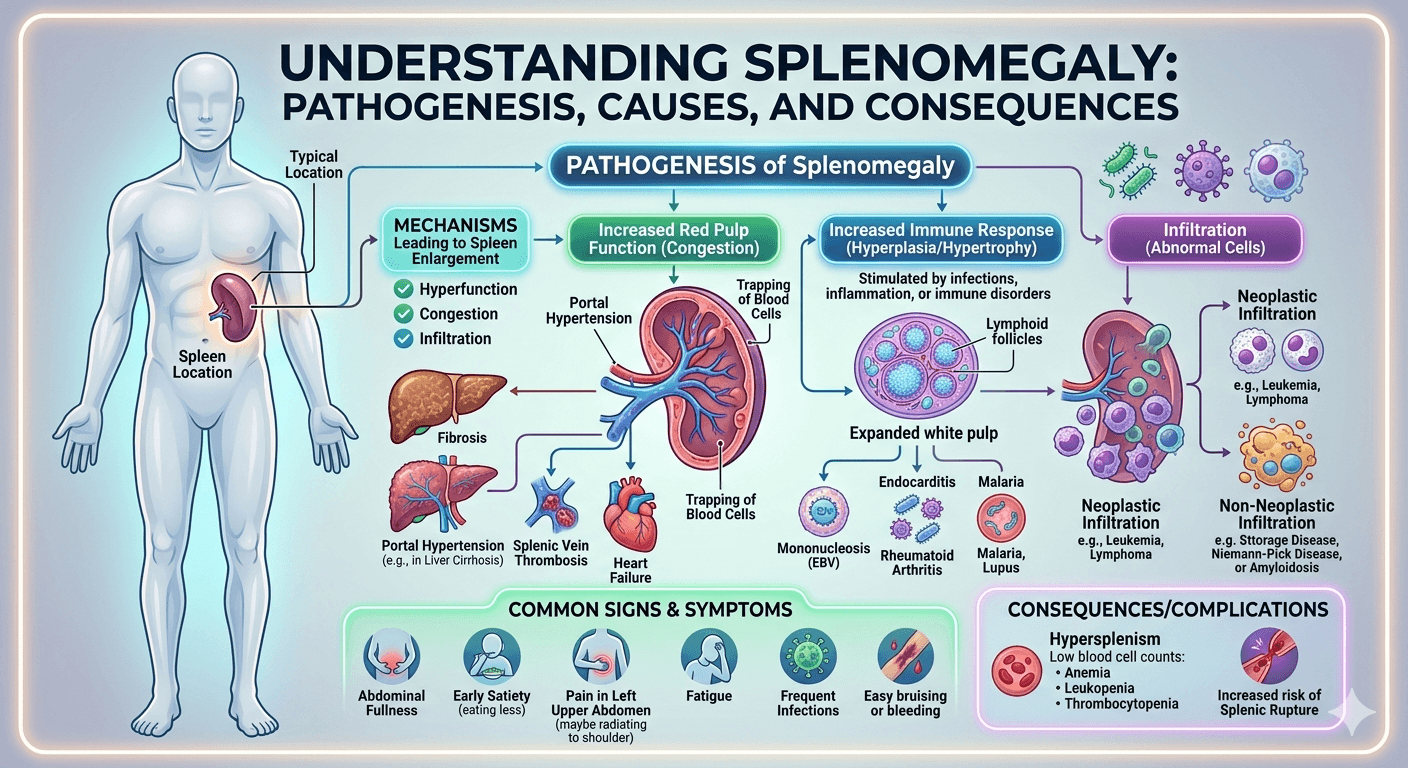
Splenomegaly refers to an abnormal enlargement of the spleen, an organ located in the upper left part of the abdomen that plays a key role in filtering blood and supporting the immune system. It is not a disease itself but a sign of underlying conditions such as infections (like malaria or mononucleosis), liver diseases (such as cirrhosis), blood disorders, or cancers like leukemia and lymphoma. Symptoms may include a feeling of fullness in the left upper abdomen, fatigue, anemia, or frequent infections. Diagnosis typically involves physical examination and imaging tests, while treatment focuses on managing the underlying cause.
1. What is splenomegaly?
Splenomegaly means enlargement of the spleen, an organ located in the upper left side of the abdomen, just below the ribs. Normally, the spleen is about the size of a fist, but in certain diseases it can become significantly larger. An enlarged spleen is not a disease itself it’s usually a sign of another underlying condition.
2. What does the spleen do in the body?
The spleen has several vital functions:
- Filters old or damaged blood cells from circulation.
- Stores blood components, especially platelets and white blood cells.
- Supports the immune system by producing antibodies and fighting infections.
- Helps recycle iron from red blood cells.
Because it is highly vascular (contains lots of blood), the spleen can enlarge when these functions are overactive or disrupted.
3. What are the common causes of splenomegaly?
Splenomegaly can result from a wide range of conditions. The main categories include:
| Category | Examples |
| Infections | Viral (EBV/mononucleosis, CMV, HIV), Bacterial (endocarditis, brucellosis), Parasitic (malaria, leishmaniasis) |
| Blood disorders | Hemolytic anemias, thalassemia, sickle cell disease (early stages) |
| Cancers | Lymphomas, leukemias, myelofibrosis, chronic myeloid leukemia |
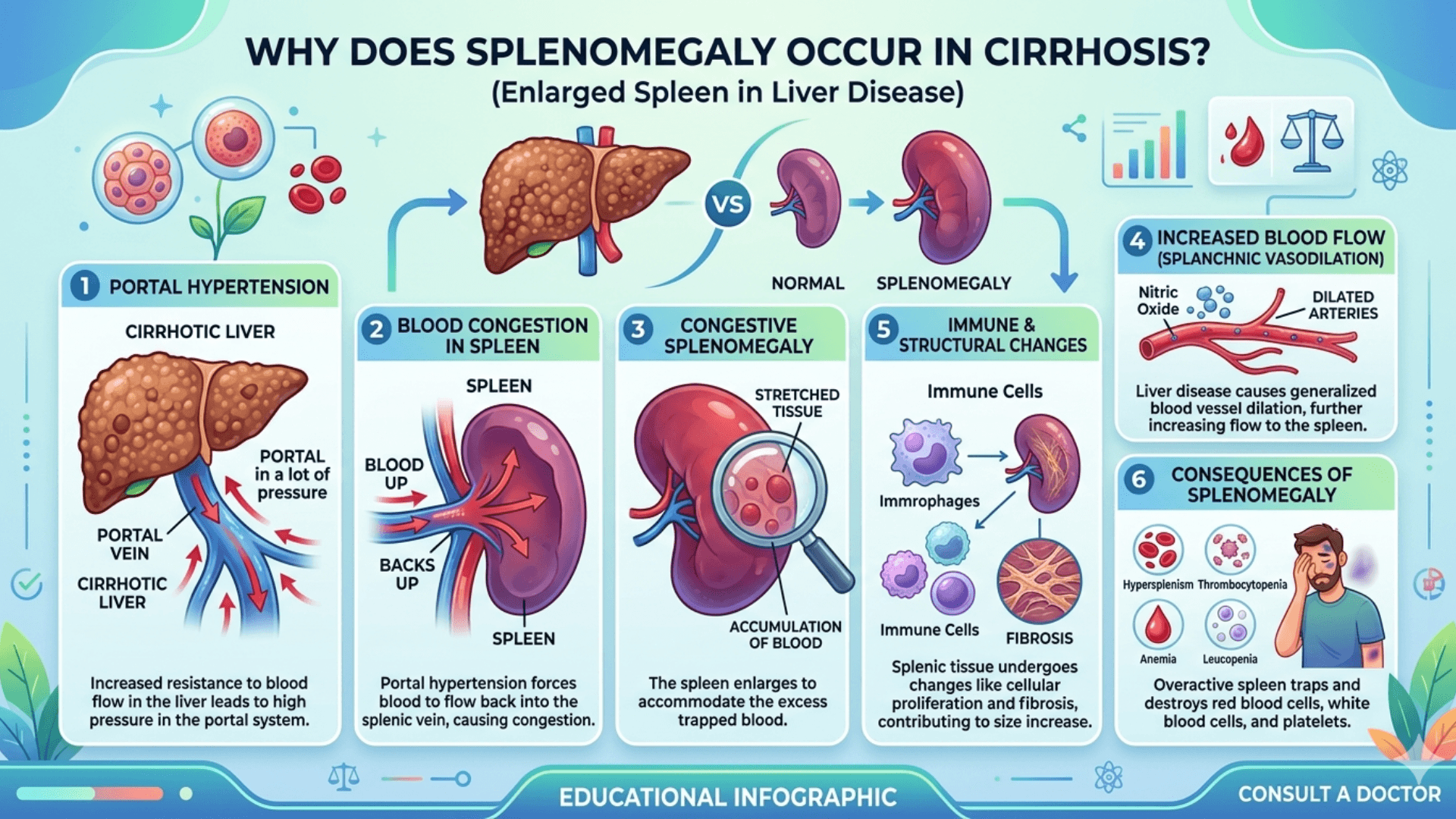
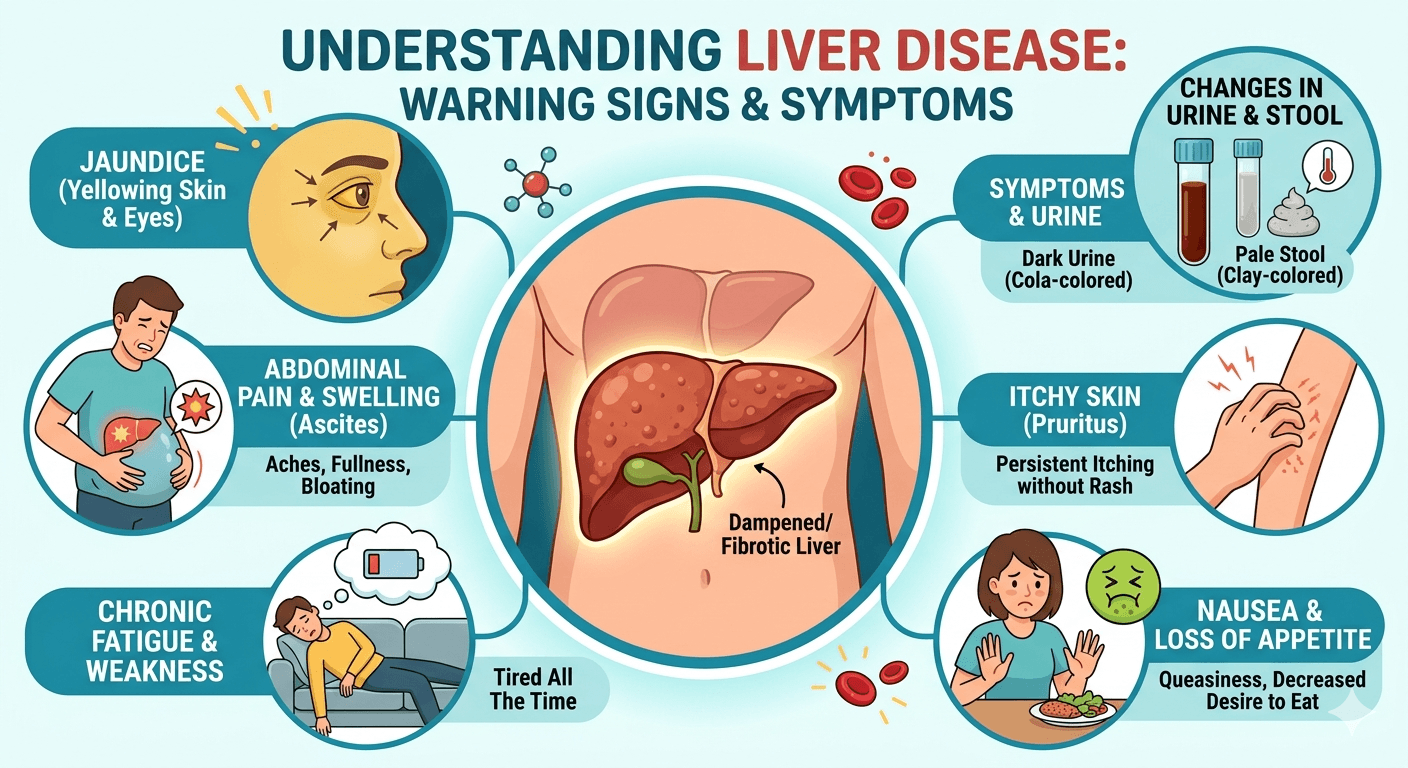
| Liver and vascular diseases | Cirrhosis with portal hypertension, splenic vein thrombosis |
| Autoimmune or inflammatory diseases | Systemic lupus erythematosus, rheumatoid arthritis (Felty’s syndrome) |
| Metabolic or storage disorders | Gaucher disease, Niemann–Pick, Amyloidosis |
4. What symptoms can splenomegaly cause?
Many people have no symptoms until the spleen becomes very large. Common symptoms include:
- A feeling of fullness or discomfort in the upper left abdomen.
- Early satiety (feeling full quickly) due to stomach compression.
- Pain in the left shoulder or upper abdomen.
- Fatigue, pallor, or frequent infections (from anemia or low white cell counts).
- Easy bruising or bleeding (from low platelets).
5. How is splenomegaly diagnosed?
Diagnosis usually starts with a clinical examination and is confirmed with tests such as:
- Physical exam: Palpation of the spleen below the left rib cage.
- Ultrasound or CT scan: Confirms size and appearance of the spleen.
- Blood tests (CBC, liver tests): To check for anemia, infection, or blood cell abnormalities.
- Bone marrow or serologic tests: If cancer, infection, or autoimmune causes are suspected.
6. What is hypersplenism, and how is it related?
Hypersplenism refers to an overactive spleen that destroys blood cells too rapidly. It often occurs in chronic splenomegaly. The result can be:
- Anemia (low red cells)
- Leucopenia (low white cells)
- Thrombocytopenia (low platelets)
Treatment focuses on managing the underlying cause, and in severe cases, partial or total splenectomy may be required.
7. Is splenomegaly dangerous?
An enlarged spleen can be dangerous because:
- It can rupture easily, especially after trauma, causing internal bleeding.
- It may trap and destroy blood cells, leading to low counts and complications.
- The underlying disease (infection, cancer, liver disease) can be serious.
Patients with splenomegaly should avoid contact sports or heavy trauma until the cause is identified and treated.
8. How is splenomegaly treated?
Treatment depends on the underlying cause, not the size of the spleen itself. Examples include:
- Infections: Appropriate antibiotics, antivirals, or antiparasitic therapy.
- Autoimmune diseases: Corticosteroids or immunosuppressants.
- Blood cancers: Chemotherapy, targeted therapy, or JAK inhibitors (for myelofibrosis).
- Portal hypertension: Management of liver disease and control of varices.
- Surgical option (splenectomy): For trauma, severe hypersplenism, or specific hematologic disorders (e.g., hereditary spherocytosis, refractory immune thrombocytopenia).
9. When is splenectomy (spleen removal) needed?
Splenectomy is recommended when:
- The spleen is causing severe pain, early satiety, or compression symptoms.
- Cytopenias (low blood counts) due to hypersplenism are severe or unresponsive to medical therapy.
- Certain diseases (e.g., hereditary spherocytosis, ITP, lymphoma) require removal for cure or control.
However, splenectomy increases infection risk, so it’s only done when clearly indicated.
10. What are the risks after splenectomy?
Without a spleen, the body becomes more susceptible to infections by encapsulated bacteria such as:
- Streptococcus pneumoniae
- Haemophilus influenzae type b
- Neisseria meningitidis
This can lead to overwhelming post-splenectomy infection (OPSI), which is rare but life-threatening. Preventive strategies include vaccination and prompt treatment of any fever.
11. What vaccines are needed after spleen removal or dysfunction?
Vaccinations should be given before or shortly after splenectomy, and repeated as needed:
- Pneumococcal vaccines PCV13/15/20 and PPSV23 boosters.
- Meningococcal vaccines both ACWY and B types.
- Haemophilus influenzae type b (Hib) vaccine.
- Annual influenza vaccine.
These vaccines significantly reduce infection risk in asplenic or hyposplenic patients.
12. What precautions should I take if I have an enlarged spleen?
- Avoid contact sports or heavy lifting to prevent rupture.
- Seek medical advice for any fever, sore throat, or infection symptoms.
- Stay up to date with vaccinations.
- Inform healthcare providers about your splenic condition before surgeries or medical treatments.
- Wear a medical alert bracelet if you have no spleen or functional asplenia.
13. Can the spleen return to normal size?
Yes if the underlying condition is successfully treated (e.g., infection cleared, inflammation resolved, blood disorder managed), the spleen may shrink back to its normal size. However, in chronic or infiltrative diseases (like myelofibrosis or storage disorders), enlargement may persist.
14. What happens if splenomegaly is left untreated?
Ignoring splenomegaly can lead to serious complications:
- Splenic rupture (medical emergency with internal bleeding).
- Severe anemia or thrombocytopenia (risk of bleeding or infection).
- Progression of the underlying disease (cancer, infection, liver failure).
Early diagnosis and management are essential to prevent long-term complications.
15. Which doctor should I see for splenomegaly?
Initial evaluation can be done by a primary care physician, but depending on the cause, you may be referred to:
- Hematologist – for blood disorders or malignancies.
- Gastroenterologist / Hepatologist for liver disease and portal hypertension.
- Infectious disease specialist for parasitic or chronic infections.
- Surgeon if splenectomy or biopsy is required.
16. What is the outlook for people with splenomegaly?
The prognosis depends entirely on the underlying cause:
- Infectious causes (like mononucleosis or malaria) often resolve completely.
- Chronic hematologic or neoplastic causes require ongoing management.
- Patients without a spleen can live normal, healthy lives with proper vaccinations and preventive care.
Key Takeaway
Splenomegaly is a symptom of an underlying condition, not a standalone disease.
Early evaluation, accurate diagnosis, and preventive care especially against infections are essential for long-term health and safety.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice.