A Detailed Medical Guide
Introduction
The kidneys play a vital role in keeping the body balanced. They do this by filtering our blood, regulating fluids and electrolytes, and flushing out waste.
Understand Nephritic and Nephrotic Syndrome with this comprehensive guide covering causes, symptoms, diagnosis, treatment, and key differences. Learn how Nephritic and Nephrotic Syndrome affect kidney function and what patients and medical students need to know.
This comprehensive guide covers the causes, symptoms, diagnosis, and treatment of both syndromes Nephritic syndrome and Nephrotic syndrome.
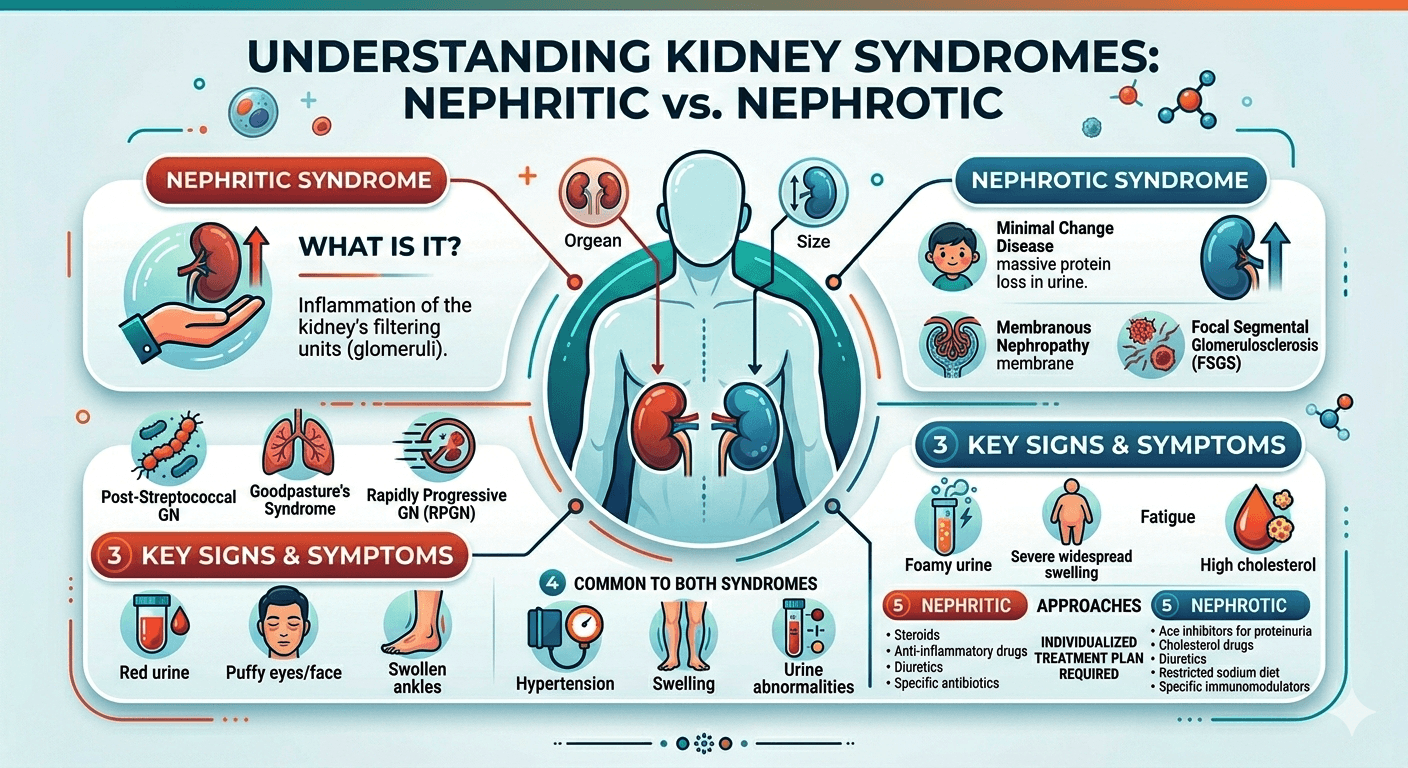
Conditions that affect the glomeruli microscopic filtration structures found in the kidney typically manifest as either nephritic syndrome or nephrotic syndrome.
While having an identical underlying structure, these two syndromes differ drastically in terms of the pathology, symptoms, laboratory findings, and management. The ability to distinguish between these two syndromes is an important skill for anyone interested in the physiology of kidney diseases.
What Is a Glomerulus?
The Glomerulus is a ball-like structure composed of capillaries that filters the blood in the kidney. It allows blood to flow out of the kidney while holding back the cells and proteins.
Glomerular filtration barrier includes the following layers:
1. Fenestrated endothelium.
2. Glomerular basement membrane (GBM)
3. Slit-diaphragm podocytes.
Damage to different components of this barrier results in distinct clinical syndromes.
Nephritic Syndrome
Definition
It is a medical syndrome marked by inflammation of the glomerulus, hence disrupting the filtration process and allowing red blood cells to appear in urine.
Features of Nephritic Syndrome
- Hematuria
- Oliguria
- Hypertension
- Mild to moderate proteinuria
- Azotemia
- Edema
Pathophysiology of Nephritic Syndrome
Glomerulonephritis develops due to inflammation of the glomeruli, which disrupts normal kidney filtration and may lead to progressive kidney damage.
Immune complexes, antibodies, and the cellular immune system cause damage to the endothelial cells lining the glomerular capillary. There are several consequences, including:
- Decreased glomerular filtration rate
- Hematuria caused by leakage of the red blood cells into the urine
- Natriuresis and water retention
- Activating the RAAS
Consequently, there is hypertension and swelling.
Clinical Presentation of Nephritic Syndrome
1. Hematuria
The hallmark of nephritic syndrome.
The color of urine appears:
- Cola-colored
- Tea-colored
- Smoky brown
Under microscopy, one can see:
- Dysmorphic red blood cells
- Blood casts in the urine
2.Oliguria
There is oliguria due to low GFR.
3.Hypertension
Retention of fluids increases the intravascular volume resulting in high BP(Hypertension)
4.Edema
This is usually mild and usually seen on:
- Facial
- Lids
- Peri-orbital areas
5. Azotemia
High levels of serum urea and creatinine
Causes of Nephritic Syndrome
Post Streptococcal Glomerulonephritis (PSGN)
Develops after infection with a nephritogenic strain of Group A Streptococcus.
Common in children.
IgA Nephropathy (Berger Disease)
It is the most common form of primary glomerulonephritis.
Deposition of IgA in the mesangium is its hallmark.
Rapidly Progressive Glomerulonephritis (RPGN)
It is a severe type that leads to the quick progression of renal failure.
Some of its causes include:
- Anti-GBM disease
- ANCA Vasculitis
- Lupus nephritis
Lupus Nephritis
An important complication of SLE.
Membranoproliferative Glomerulonephritis (MPGN)
Laboratory Abnormalities in Nephritic Syndrome
Urinalysis
Abnormal findings include:
- Hematuria
- RBC casts
- Proteinuria
Blood Tests
- Elevated creatinine
- Elevated blood urea nitrogen (BUN)
- Reduced complement levels (for some causes)
Kidney Biopsy
- Hypercellularity
- Immune complex deposition
- Crescent formation
Nephrotic Syndrome
Description
Nephrotic syndrome is caused by increased permeability of the glomerular filtration barrier, leading to massive protein loss through the urine.
Diagnosis Criteria
- Proteinuria of >3.5g/day
- Hypoalbuminemia
- Generalized edema
- Hyperlipidemia
- Lipiduria
Nephrotic Syndrome Pathophysiology
Damage occurs to podocytes and glomerular basement membranes.
Consequences include:
1. Massive urinary protein loss
2. Decreased plasma oncotic pressure
3. Fluid movement from capillaries to interstitial spaces
4. Edema formation
The liver responds by synthesizing more proteins and lipoproteins leading to hyperlipidemia.
Clinical Manifestations of Nephrotic Syndrome
1. Massive proteinuria
Excretion of more than 3.5g of protein daily.
2. Edema formation
Known as anasarca.(anasarca is a medical condition in which excessive fluid buildup throughout the body, causing widespread swelling of the skin and tissues.)
Sites include:
- Face
- Legs
- Abdomen
- Scrotum
3. Hypoalbuminemia
Decreased serum albumin due to excessive urinary losses.
4. Hyperlipidemia
Elevated level of cholesterol and triglycerides is common.
5. Lipiduria
Microscopy of urine reveals:
- Oval fat bodies
- Fatty casts
Producing the characteristic “Maltese cross” when viewed under polarized light.
Causes of Nephrotic Syndrome
Minimal Change Disease (MCD)
The most common cause in children.
Features:
• Normal light microscopy
• Podocyte foot process effacement on electron microscopy
Focal Segmental Glomerulosclerosis (FSGS)
Commonly seen in adults.
Associated with:
• HIV infection
• Obesity
• Sickle cell disease
Membranous Nephropathy
Common cause in older adults.
Associated with anti-PLA2R antibodies.
Diabetic Nephropathy
The diabetes is the commonest cause of nephrotic syndrome globally.
Amyloidosis
Extracellular deposition of amyloid proteins damages the kidneys.
Complications of Nephrotic Syndrome
Thromboembolism
Deficiency of anticoagulant proteins like ant thrombin III makes it easier to form clots.
Complications of nephrotic syndrome include:
- Renal vein thrombosis
- Deep vein thrombosis
- Pulmonary embolism
Infections
Due to loss of immunoglobulins, there is increased susceptibility to infections.
Examples of such infections include:
- Pneumonia
- Cellulitis
- Peritonitis
Malnutrition
Persistent protein loss causes muscle wastage.
Acute kidney injury
May occur in severe cases.
Laboratory Abnormalities in Nephrotic Syndrome
Urinalysis
Massive proteinuria
Fatty casts
Oval fat bodies
Blood Tests
Common findings include:
| Test Result |
| Serum albumin Decreased |
| Cholesterol Increased |
| Triglycerides Increased |
Creatinine Variable
Kidney Biopsy
Required in adults to determine the underlying cause.
Difference Between Nephritic and Nephrotic Syndrome
| Feature | Nephritic Syndrome | Nephrotic Syndrome |
| Definition | A glomerular disorder characterized primarily by inflammation and hematuria. | A glomerular disorder characterized primarily by massive protein loss in the urine. |
| Primary Pathology | Inflammation of the glomeruli. | Increased permeability of the glomerular filtration barrier. |
| Proteinuria | Mild to moderate (<3.5 g/day). | Severe (>3.5 g/day). |
| Hematuria | Prominent; urine may appear smoky, tea-colored, or cola-colored. | Usually absent or microscopic if present. |
| Red Blood Cell Casts | Common and characteristic. | Rare. |
| Edema | Mild to moderate, often around the eyes. | Severe, generalized edema (anasarca). |
| Blood Pressure | Frequently elevated (hypertension). | Usually normal or mildly elevated. |
| Serum Albumin | Slightly reduced or normal. | Markedly decreased (Hypoalbuminemia). |
| Serum Lipids | Usually normal. | Elevated cholesterol and triglycerides (hyperlipidemia). |
| Urine Appearance | Dark, smoky, or bloody. | Frothy or foamy due to excess protein. |
| Kidney Function | Often reduced, with decreased glomerular filtration rate (GFR). | Usually preserved initially. |
| Fluid Retention | Present due to reduced kidney function. | Marked due to low plasma oncotic pressure. |
| Risk of Blood Clots | Less common. | Increased risk because of loss of anticoagulant proteins in urine. |
| Common Causes | Post-streptococcal glomerulonephritis, IgA nephropathy, rapidly progressive glomerulonephritis, lupus nephritis. | Minimal change disease, focal segmental glomerulosclerosis (FSGS), membranous nephropathy, diabetic nephropathy. |
| Key Clinical Features | Hematuria, hypertension, oliguria, and mild edema. | Massive proteinuria, severe edema, hypoalbuminemia, and hyperlipidemia. |
| Treatment Focus | Controlling inflammation, blood pressure, and treating the underlying cause. | Reducing proteinuria, managing edema, preventing complications, and treating the underlying disease. |
Diagnostic Approaches
History
The essential queries include:
- Any recent infection?
- Indications of autoimmune illness
- The patient’s medication list
- History of any hereditary condition?
Physical examination
Check for:
- Level of blood pressure
- The extent of edema
- Systemic disease signs
Laboratory Tests
Suggested investigations:
| Urinalysis |
| Measurement of urine proteins |
| Serum creatinine |
| Serum albumin |
| Kidney function test (KFT) |
| Liver function test |
| LDH level |
| Lipid profile |
| D-dimer test |
| Testing of complement levels |
| Anti nuclear antibody (ANA) |
| Anti-neutrophil cytoplasmic antibodies (ANCA) |
| Anti GBM antibodies |
Imaging
- Ultrasound (USG) whole abdomen
- CT abdomen (as decided by physician)
- Renal biopsy
Generally aids in making definitive diagnosis
Approach to Treatment
Approach to Nephritic Syndrome
Treat based on cause
General Approach:
- Treatment of hypertension
- Limited intake of fluids
- Limitation in sodium
- Use of diuretics
Specific approach for the particular disease may include:
- Steroids
- Cytotoxic therapy
- Rituximab
- Plasmapheresis
(Treatment entirely depends upon physician)
Approach to Nephrotic Syndrome
General Approach
- Limit salt consumption
- Administration of diuretics
- ACE inhibitors
- ARBs
Hyperlipidemia Management
Use statins when indicated
Prevention of thrombosis
Indicated in high-risk cases
Specific treatment depends upon diagnosis
Steroids, calcineurin inhibitors, rituximab, etc.
Prognosis
Prognosis is based upon cause.
Good prognosis
- Minimal change disease
- Post Streptococcal Glomerulonephritis
Average prognosis
- IgA nephropathy
- Membranous nephropathy
conclusion
Both nephritic and nephrotic syndrome are important types of kidney diseases that occur due to injury to glomeruli, but there are significant differences in their development, symptoms, lab results, and treatment modalities. First of all, nephritic syndrome is caused by inflammation of glomeruli, which produces symptoms like hematuria, hypertension, and decreased functioning of kidneys. Nephrotic syndrome, on the other hand, occurs when the permeability of glomeruli increases, resulting in heavy proteinuria, edema, Hypoalbuminemia, and hyperlipidemia.
Understanding the difference between these syndromes is key to accurate diagnostics, effective treatment, and even preventing serious complications in the form of chronic kidney disease or renal failure. The knowledge about pathogenesis and signs of nephritic and nephrotic syndromes plays an especially vital role for future medical professionals. Patients should be informed about symptoms like edema, abnormal urination, high blood pressure, or unusual tiredness. With proper care, many cases of nephritic or nephrotic syndromes can be successfully managed.
Frequently Asked Questions (FAQs)
1. What is the easiest way to differentiate nephritic and nephrotic syndrome?
Nephritic syndrome presents with hematuria and inflammation, while nephrotic syndrome presents with massive proteinuria and generalized edema.
2. Why does nephrotic syndrome cause hyperlipidemia?
The liver compensates for protein loss by increasing synthesis of lipoproteins, resulting in elevated cholesterol and triglyceride levels.
3. Are RBC casts specific for nephritic syndrome?
Yes. RBC casts strongly suggest glomerular inflammation and are a classic feature of nephritic syndrome.
4. Which syndrome causes more severe edema?
Nephrotic syndrome causes more severe edema because of significant hypoalbuminemia.
5. What is the most common nephrotic syndrome in children?
Minimal Change Disease is the most common cause in children.
6. Can nephritic syndrome progress to kidney failure?
Yes. Severe forms such as rapidly progressive glomerulonephritis can lead to acute or chronic kidney failure if untreated.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment. Always seek the guidance of a qualified healthcare professional regarding any medical condition or health-related concerns. The author and publisher are not responsible for any actions taken based on the information presented in this article.