Chest Pain Causes, Diagnosis, and a Practical Clinical Approach
Learn about chest pain causes, diagnosis, and a practical clinical approach. This comprehensive guide explains symptoms, evaluation, investigations, and management strategies for both patients and medical students.
Introduction
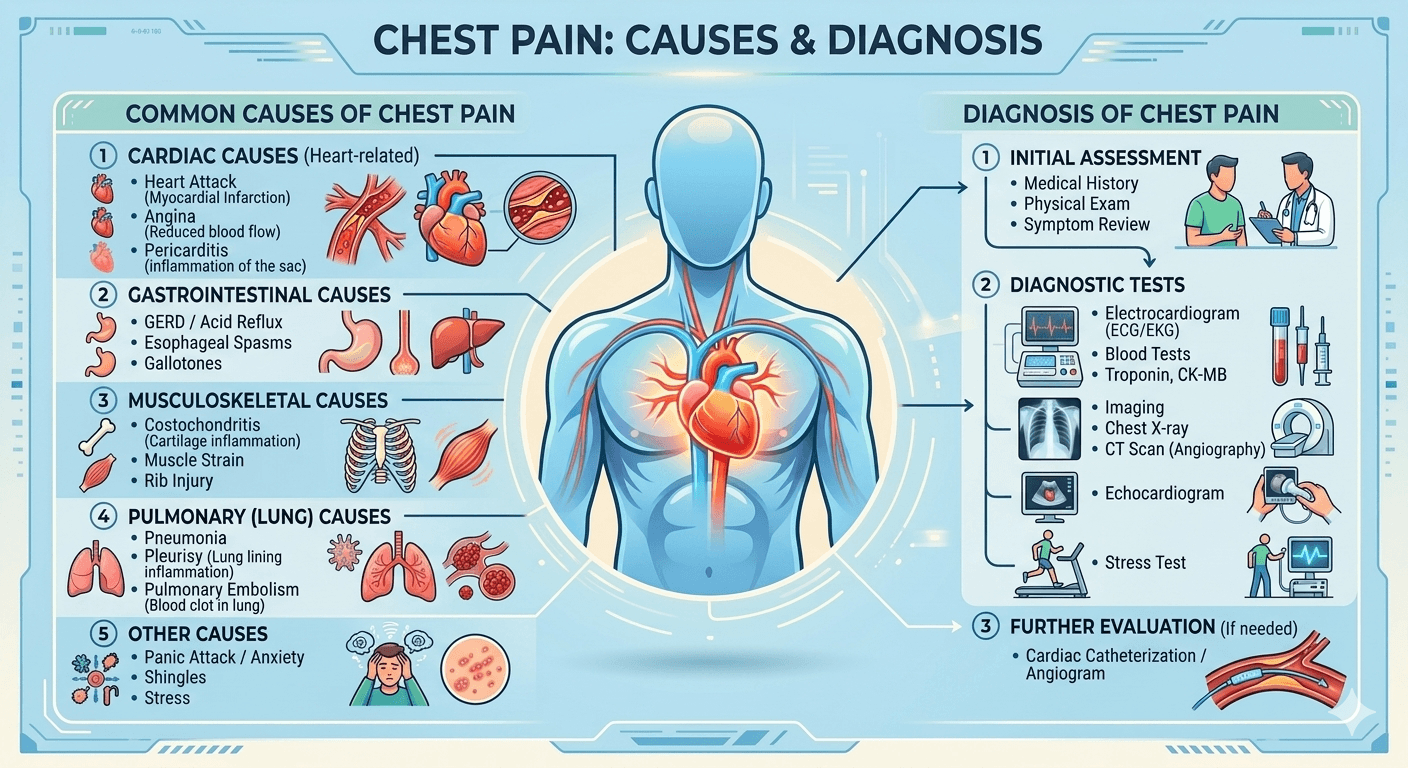
Chest pain is probably one of the most common and worrying signs seen in medicine. For patients, it may provoke fear about having a myocardial infarction. As far as medical doctors and interns are concerned, chest pain poses a diagnostic issue since it may have both benign and lethal causes.
As a doctor, one of the first things I tell my intern colleagues is that not all chest pains are of cardiac origin; however, any complaint of chest pain must be approached thoughtfully, which may help save a person’s life while avoiding false worries and expensive tests.
This article describes an accessible yet informative guide to chest pain, outlining possible causes and the process of diagnosing it.
Understanding Chest Pain
Chest pain refers to any discomfort, pressure, tightness, burning, or pain felt between the neck and upper abdomen. The sensation can vary significantly among individuals.
Patients may describe chest pain as:
- Sharp or stabbing
- Dull aching
- Crushing pressure
- Burning sensation
- Tightness or squeezing
- Heaviness on the chest
- Discomfort radiating to the arm, jaw, back, or neck
The character of pain often provides valuable diagnostic clues but should never be used in isolation to determine the cause.
Why Chest Pain Occurs
The chest contains multiple structures capable of generating pain:
| Structure | Possible Cause of Pain |
| Heart | Angina, heart attack, pericarditis |
| Blood vessels | Aortic dissection, pulmonary embolism |
| Lungs | Pneumonia, pneumothorax |
| Esophagus | Acid reflux, esophageal spasm |
| Muscles and ribs | Muscle strain, costochondritis |
| Nerves | Shingles, nerve irritation |
| Psychological factors | Anxiety, panic attacks |
Understanding the anatomy of the chest helps clinicians systematically evaluate potential sources of pain.
Life-Threatening Causes of Chest Pain
The first responsibility of any healthcare provider is identifying dangerous conditions that require immediate intervention.
1. Acute Coronary Syndrome (ACS)
Acute coronary syndrome includes:
- Unstable angina
- Non-ST elevation myocardial infarction (NSTEMI)
- ST-elevation myocardial infarction (STEMI)
Typical Features
- Central chest pressure
- Tightness or heaviness
- Radiation to left arm, jaw, or shoulder
- Associated sweating
- Nausea
- Shortness of breath
Risk Factors
- Hypertension
- Diabetes
- Smoking
- High cholesterol
- Family history of heart disease
- Advanced age
Patients with ACS may not always present classically. Women, older adults, and diabetic patients frequently have atypical symptoms.
2. Aortic Dissection
Aortic dissection occurs when a tear develops within the wall of the aorta.
Classic Presentation
- Sudden severe chest pain
- Tearing or ripping sensation
- Pain radiating to the back
- Blood pressure differences between arms
This condition is a true medical emergency with high mortality if untreated.
3. Pulmonary Embolism (PE)
Pulmonary embolism results from a blood clot blocking arteries in the lungs.
Common Symptoms
- Sudden chest pain
- Shortness of breath
- Rapid heart rate
- Coughing blood
- Low oxygen levels
Risk Factors
- Recent surgery
- Prolonged immobility
- Cancer
- Pregnancy
- Deep vein thrombosis
4. Pneumothorax
A pneumothorax occurs when air enters the pleural space surrounding the lung.
Symptoms
- Sudden sharp chest pain
- Difficulty breathing
- Reduced breath sounds on examination
Young, tall individuals and patients with chronic lung disease are at increased risk.
5. Cardiac Tamponade
Cardiac tamponade results from fluid accumulation around the heart.
Key Findings
- Chest discomfort
- Low blood pressure
- Elevated neck veins
- Shortness of breath
Prompt recognition is essential because untreated tamponade can rapidly become fatal.
Common Non-Life-Threatening Causes of Chest Pain
Fortunately, many cases of chest pain arise from less dangerous conditions.
Gastroesophageal Reflux Disease (GERD)
Acid reflux is one of the most frequent causes of chest discomfort.
Symptoms
- Burning behind the breastbone
- Sour taste in the mouth
- Symptoms after meals
- Worse when lying down
GERD often mimics cardiac chest pain, making careful evaluation important.
Costochondritis
Costochondritis is inflammation of the cartilage connecting ribs to the breastbone.
Clinical Features
- Localized chest pain
- Pain reproducible by pressing the chest wall
- Worse with movement
This condition is generally benign and self-limiting.
Muscle Strain
Chest wall muscles may become strained following:
- Heavy lifting
- Intense exercise
- Persistent coughing
- Trauma
Pain usually worsens with movement and improves with rest.
Panic Attacks and Anxiety
Psychological causes frequently contribute to chest pain.
Associated Symptoms
- Rapid heartbeat
- Hyperventilation
- Dizziness
- Fear of dying
- Tingling sensations
Although anxiety-related chest pain is not usually dangerous, a medical assessment should exclude physical causes before making this diagnosis.
Pleuritis
Inflammation of the pleura, the membrane covering the lungs, causes:
- Sharp chest pain
- Pain with deep breathing
- Pain during coughing
Viral infections are common causes.
Clinical Evaluation of Chest Pain
A structured clinical approach is critical.
Step 1: Immediate Assessment
First, the clinician determines whether the patient is stable.
Assess:
- Airway
- Breathing
- Circulation
- Oxygen saturation
- Blood pressure
- Heart rate
Any instability requires urgent intervention.
Step 2: Focused History Taking
A detailed history often provides the most essential diagnostic clues.
Medical students frequently use the mnemonic OPQRST.
O – Onset
- When did the pain start?
- Sudden or gradual?
P – Provocation
- What makes it better or worse?
Q – Quality
- Sharp?
- Burning?
- Crushing?
R – Radiation
- Does it spread anywhere?
S – Severity
- Pain scale from 0 to 10
T – Timing
- Constant or intermittent?
Additional Important Questions
Associated Symptoms
Ask about:
- Shortness of breath
- Sweating
- Nausea
- Palpitations
- Fever
- Cough
- Syncope
Risk Factors
Assess for:
- Smoking
- Hypertension
- Diabetes
- Hyperlipidemia
- Family history
Physical Examination
A careful examination follows.
General Appearance
Observe whether the patient appears:
- Comfortable
- Anxious
- Distressed
- Sweaty
Vital Signs
Document:
- Temperature
- Pulse
- Respiratory rate
- Blood pressure
- Oxygen saturation
Abnormal vital signs often provide diagnostic clues.
Cardiovascular Examination
Evaluate for:
- Heart murmurs
- Extra heart sounds
- Pericardial rub
- Jugular venous distension
Respiratory Examination
Assess:
- Breath sounds
- Crackles
- Wheezing
- Reduced air entry
Chest Wall Examination
Palpate the chest wall.
Pain reproducible by palpation often suggests a musculoskeletal source, although this finding does not completely exclude cardiac disease.
Diagnostic Investigations
Investigations should be guided by clinical suspicion.
Electrocardiogram (ECG)
The ECG is one of the most important initial tests.
It can identify:
- Heart attacks
- Arrhythmias
- Pericarditis
- Ischemia
An ECG should ideally be obtained within minutes of presentation when cardiac causes are suspected.
Cardiac Biomarkers
Troponin
Troponin is the preferred biomarker for myocardial injury.
Elevated levels suggest:
- Heart attack
- Myocarditis
- Severe cardiac stress
Serial measurements improve diagnostic accuracy.
Chest X-Ray
Chest radiography can reveal:
- Pneumonia
- Pneumothorax
- Heart enlargement
- Pleural effusions
Blood Tests
Common laboratory investigations include:
- Complete blood count
- Electrolytes
- Kidney function
- Lipid profile
- Trop T and Trop I
- RBS, HbA1c
- D-dimer
- Inflammatory markers
Echocardiography
Echocardiography evaluates:
- Cardiac function
- Valve disease
- Pericardial effusion
- Structural abnormalities
CT Imaging
CT scans are especially useful for:
CT Pulmonary Angiography
Used to diagnose pulmonary embolism.
CT Aortography
Used to diagnose aortic dissection.
Stress Testing
Stress tests help evaluate coronary artery disease when immediate danger has been excluded.
Methods include:
- Exercise treadmill testing
- Stress echocardiography
- Nuclear imaging
A Practical Clinical Approach for Medical Students
When evaluating chest pain, think systematically.
First Question: Is the Patient Stable?
Check:
- Blood pressure
- Oxygenation
- Mental status
Instability demands immediate action.
Second Question: Could This Be One of the Deadly Five?
Always consider:
- Acute coronary syndrome
- Aortic dissection
- Pulmonary embolism
- Pneumothorax
- Cardiac tamponade
These conditions must be excluded first.
Third Question: What Does the History Suggest?
Seek patterns.
| Symptom Pattern | Possible Diagnosis |
| Exertional pressure | Angina |
| Burning after meals | GERD |
| Sharp pain with inspiration | Pleuritis |
| Reproducible tenderness | Costochondritis |
| Sudden tearing pain | Aortic dissection |
Fourth Question: What Investigations Are Needed?
Tailor testing based on clinical probability rather than ordering every available investigation.
This principle improves efficiency and patient safety.
When Should Patients Seek Emergency Care?
Patients should seek immediate medical attention if chest pain is associated with:
- Shortness of breath
- Sweating
- Fainting
- Radiation to arm or jaw
- Sudden severe onset
- Known heart disease
- Persistent symptoms
When in doubt, it is safer to seek emergency evaluation.
Preventing Serious Causes of Chest Pain
Many cardiac causes are preventable through lifestyle modifications.
Key Preventive Measures
Healthy Diet
Focus on:
- Fruits
- Vegetables
- Whole grains
- Lean proteins
Regular Exercise
Aim for at least 150 minutes of moderate exercise weekly.
Smoking Cessation
Stopping smoking significantly reduces cardiovascular risk.
Blood Pressure Control
Regular blood pressure monitoring and, if hypertension is present, appropriate treatment are essential.
Diabetes Management
Proper control of diabetes helps preserve blood vessel function and lowers the risk of heart disease.
Frequently Asked Questions (FAQs)
Is all chest pain a heart attack?
No. Many causes of chest pain are unrelated to the heart, including acid reflux, muscle strain, and anxiety. However, serious cardiac causes must always be considered.
Can anxiety really cause chest pain?
Yes. Anxiety and panic attacks can produce significant chest discomfort, palpitations, and shortness of breath that closely mimic heart disease.
What is the first test performed for suspected cardiac chest pain?
An electrocardiogram (ECG) is typically the first diagnostic test because it can rapidly identify life-threatening cardiac conditions.
How can I tell if chest pain is muscular?
Musculoskeletal pain is often localized, worsens with movement, and may be reproducible when pressing on the affected area.
Why do doctors measure troponin levels?
Troponin is released when heart muscle is damaged. Elevated levels help diagnose heart attacks and other cardiac conditions.
Should young, healthy individuals worry about chest pain?
Although serious causes are less common in younger individuals, chest pain should still be evaluated when severe, persistent, or accompanied by concerning symptoms.
Conclusion
Despite all advances in clinical medicine, chest pain continues to be one of the vital signs that may signify conditions starting from innocuous musculoskeletal problems up to potentially fatal pathologies. From the patient’s perspective, knowledge of the variety of factors underlying this condition helps alleviate any concerns but at the same time motivates one to see the doctor if needed. For a medical student, however, the development of such an approach in which he starts with assessing his patient’s stability, identifying life-threatening pathologies, taking a history, examining a patient, and conducting relevant investigations is crucial for competent work.
This basic rule is quite straightforward: first you exclude serious pathology, and then you continue narrowing down the list of differential diagnoses.
Additional Resources
- American Heart Association (AHA)
- World Health Organization (WHO)
- Centers for Disease Control and Prevention (CDC)
- National Institutes of Health (NIH)
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment.