Gastropathy vs. Gastritis: Key Differences Explained
Gastropathy vs. Gastritis: Key Differences Explained clears up the frequent confusion between these two stomach conditions. While they share similar symptoms like nausea and pain, gastritis involves active stomach lining inflammation (often from infections), whereas gastropathy refers to lining damage without significant inflammation (typically caused by NSAIDs or alcohol).
Introduction
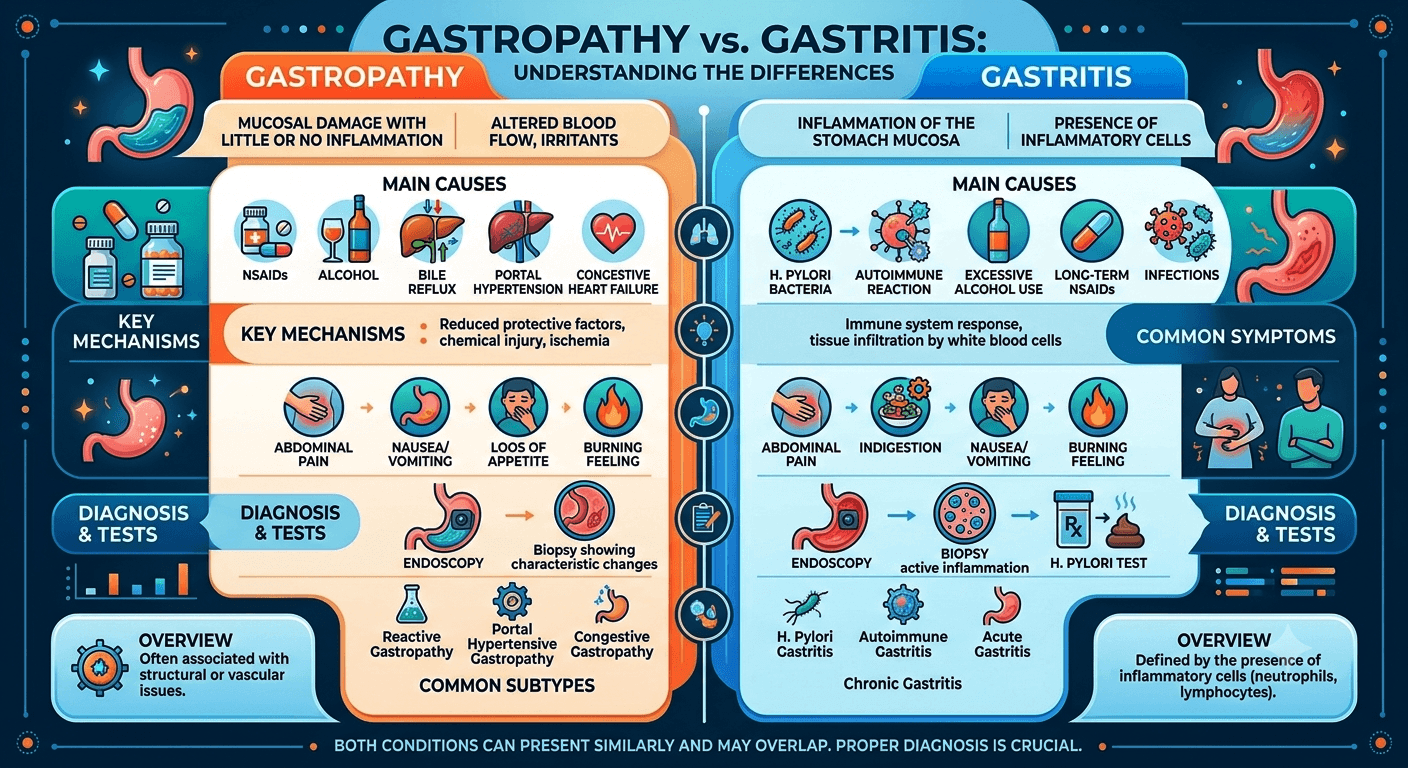
The terms Gastropathy and Gastritis are frequently used interchangeably in clinical practice and by patients, but they represent fundamentally different pathological processes. Understanding the distinction is important because the causes, microscopic findings, treatment strategies, and long-term implications may differ significantly.
Gastropathy vs. Gastritis: Key Differences Explained clears up the frequent confusion between these two stomach conditions. While they share similar symptoms like nausea and pain.
Gastritis refers specifically to inflammation of the gastric (stomach) mucosa, characterized by inflammatory cell infiltration within the stomach lining. It is therefore a disease process defined by inflammation.
Gastropathy, in contrast, refers to damage or injury to the gastric mucosa with little or no significant inflammation. It is primarily a morphological (structural) description based on endoscopic and histological findings rather than a specific inflammatory disease.
The purpose of this explanation is to clarify the key differences between gastropathy and gastritis, including their pathophysiology, causes, symptoms, diagnosis, and management.
Anatomy & Pathophysiology
Normal Anatomy of the Stomach
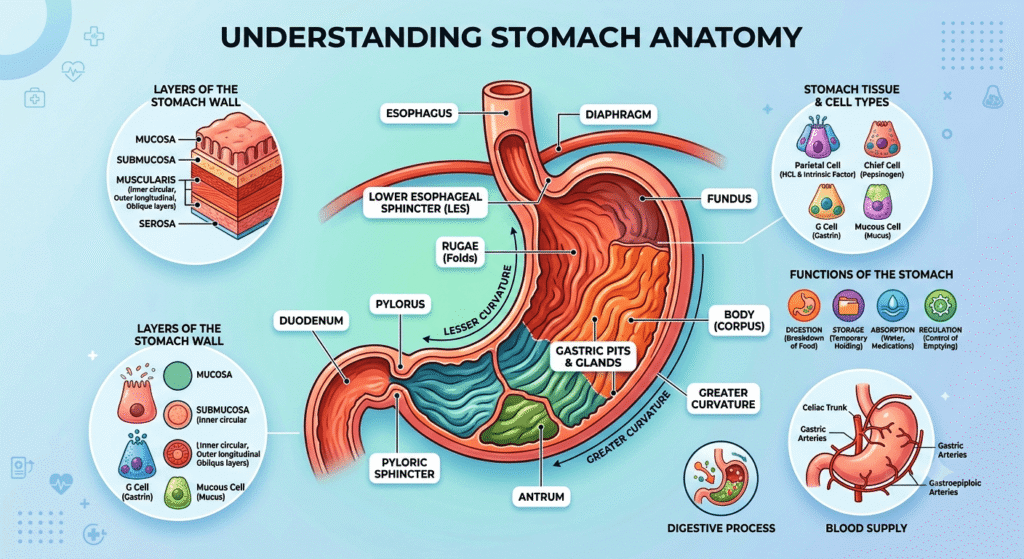
The stomach is a muscular organ located between the esophagus and the small intestine. Its primary functions include:
- Storage of food
- Mechanical digestion
- Secretion of gastric acid and digestive enzymes
- Regulation of food passage into the duodenum
The stomach wall consists of several layers:
- Mucosa—the innermost layer containing epithelial cells, gastric glands, and protective mucus-producing cells.
- Submucosa—contains blood vessels, lymphatics, and nerves.
- Muscularis propria—responsible for stomach contractions.
- Serosa—the outer covering.
The gastric mucosa is protected by a sophisticated defense system that includes:
- Mucus secretion
- Bicarbonate production
- Adequate blood flow
- Tight epithelial junctions
- Rapid cell regeneration
When these protective mechanisms fail, mucosal injury develops.
Pathophysiology of Gastritis
Gastritis is fundamentally an inflammatory disorder.
When the gastric mucosa is exposed to damaging stimuli, the immune system responds by recruiting inflammatory cells such as:
- Neutrophils
- Lymphocytes
- Plasma cells
- Macrophages
The resulting inflammation may be:
Acute Gastritis
Characterized by:
- Sudden onset
- Neutrophilic infiltration
- Mucosal edema
- Surface erosions
- Potential bleeding
Chronic Gastritis
Characterized by:
- Persistent inflammation
- Lymphocyte and plasma cell infiltration
- Progressive glandular damage
- Mucosal atrophy
- Intestinal metaplasia in some cases
Chronic inflammation can increase the risk of gastric ulcers and, in some patients, gastric cancer.
Pathophysiology of Gastropathy
Gastropathy involves epithelial injury and mucosal damage with little or no inflammatory response.
Instead of inflammation, pathological findings often include:
- Foveolar hyperplasia (elongation of gastric pits)
- Mucosal edema
- Vascular congestion
- Surface epithelial degeneration
- Capillary dilation
The injury typically results from:
- Chemical irritation
- Bile reflux
- Medications
- Alcohol
- Vascular abnormalities
The classic example is reactive (chemical) gastropathy, where the stomach lining becomes damaged but inflammatory cells are largely absent. Thus, the central distinction is
| Gastritis | Gastropathy |
| Inflammatory process | Non-inflammatory mucosal injury |
| Inflammatory cells present | Minimal or absent inflammation |
| Disease diagnosis | Morphological description |
| Often immune-mediated or infectious | Often chemical, vascular, or mechanical |
Causes
Causes of Gastritis
Helicobacter pylori Infection
The most common cause worldwide is infection with the bacterium:
Helicobacter pylori Infection
This organism colonizes the gastric mucosa and triggers chronic inflammation.
Autoimmune Gastritis
An autoimmune disorder in which antibodies attack:
- Parietal cells
- Intrinsic factor
This can lead to:
- Vitamin B12 deficiency
- Pernicious anemia
- Gastric atrophy
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
Examples include:
- Aspirin
- Ibuprofen
- Naproxen
These medications impair mucosal protection and may induce inflammation.
Alcohol
Heavy alcohol consumption can directly damage the gastric mucosa and provoke gastritis.
Stress-Related Gastritis
Seen in critically ill patients with:
- Severe burns
- Trauma
- Sepsis
- Major surgery
Radiation and Chemotherapy
These therapies may injure gastric tissues and trigger inflammation.
Less Common Causes
- Viral infections
- Fungal infections
- Parasitic infections
- Crohn’s disease
- Sarcoidosis
- Eosinophilic disorders
Causes of Gastropathy
Reactive (Chemical) Gastropathy
The most common form.
Typically caused by:
- Bile reflux into the stomach
- Chronic NSAID exposure
- Alcohol use
Portal Hypertensive Gastropathy
Occurs in patients with:
Portal Hypertension
Most often due to:
- Cirrhosis
- Advanced liver disease
The increased pressure alters gastric blood flow and causes characteristic mucosal changes.
Congestive Gastropathy
Associated with:
- Heart failure
- Venous congestion
Radiation Gastropathy
Develops after radiation exposure to the stomach.
Ischemic Gastropathy
Results from reduced blood supply to gastric tissues.
Medication-Induced Gastropathy
Can occur with:
- NSAIDs
- Potassium supplements
- Iron tablets
- Certain chemotherapy agents
Symptoms
Symptoms of Gastritis
Many patients are asymptomatic, but common symptoms include:
- Upper abdominal pain
- Burning epigastric discomfort
- Nausea
- Vomiting
- Bloating
- Loss of appetite
- Early satiety
More severe cases may present with:
- Gastrointestinal bleeding
- Black stools (melena)
- Vomiting blood (hematemesis)
Chronic gastritis may also lead to:
- Fatigue
- Vitamin B12 deficiency
- Anemia
Symptoms of Gastropathy
Symptoms can overlap considerably with gastritis.
Common manifestations include:
- Indigestion
- Upper abdominal discomfort
- Bloating
- Nausea
- Early fullness after meals
- Mild epigastric pain
Some patients experience no symptoms at all.
Portal hypertensive gastropathy may present with:
- Chronic blood loss
- Iron-deficiency anemia
- Occult gastrointestinal bleeding
Acute bleeding can occur in severe cases.
Diagnosis
Clinical Evaluation
Diagnosis begins with:
- Medical history
- Medication review
- Alcohol intake assessment
- Evaluation of symptoms
- Physical examination
However, symptoms alone cannot reliably distinguish gastritis from gastropathy.
Laboratory Testing
Depending on the clinical situation, testing may include:
- Complete blood count (CBC)
- Iron studies
- Vitamin B12 levels
- Vitamin D3
- Liver function tests
- LDH
- Lipid profile
- Viral marker
- H. pylori testing
Methods for detecting H. pylori include:
- Urea breath test
- Stool antigen testing
- Biopsy testing
- Blood antibody testing
Upper Endoscopy
The most important diagnostic procedure is:
Esophagogastroduodenoscopy (EGD)
During endoscopy, physicians can evaluate:
- Erythema
- Erosions
- Ulcers
- Bleeding
- Mucosal abnormalities
Visual appearance alone may not distinguish gastritis from gastropathy.
Histopathological Examination
Biopsy is the gold standard for differentiation.
Gastritis Biopsy Findings
Demonstrates:
- Neutrophils
- Lymphocytes
- Plasma cells
- Mucosal inflammation
- Atrophy or metaplasia
Gastropathy Biopsy Findings
Shows:
- Foveolar hyperplasia
- Mucosal edema
- Vascular congestion
- Surface epithelial damage
Inflammatory cells are absent or minimal.
This histological distinction is what definitively separates gastritis from gastropathy.
Treatment
Treatment of Gastritis
Treatment depends on the underlying cause.
H. pylori Eradication
Patients with H. pylori infection require antibiotic therapy combined with acid suppression.
Acid Suppression
Common medications include:
- Proton pump inhibitors (PPIs)
- Histamine-2 receptor blockers
Examples include:
- Omeprazole
- Pantoprazole
Autoimmune Gastritis Management
Treatment focuses on:
- Vitamin B12 replacement
- Monitoring for complications
- Surveillance when indicated
Lifestyle Measures
Patients are advised to:
- Avoid excessive alcohol
- Stop smoking
- Limit gastric irritants
- Avoid unnecessary NSAID use
Treatment of Gastropathy
Management focuses on removing or correcting the underlying source of injury.
Reactive Gastropathy
Treatment includes:
- Discontinuing offending medications
- Reducing alcohol intake
- Managing bile reflux
- Acid suppression therapy when appropriate
Portal Hypertensive Gastropathy
Management focuses on reducing portal pressure.
Treatment options may include:
- Nonselective beta-blockers
- Endoscopic therapy
- Management of underlying liver disease
Ischemic or Congestive Gastropathy
Treatment addresses:
- Cardiovascular disease
- Blood flow abnormalities
- Underlying systemic conditions
Supportive Measures
General recommendations include:
- Balanced nutrition
- Avoidance of irritants
- Monitoring for bleeding
- Treatment of anemia if present
Living with Gastropathy & Gastritis
Living with either condition often requires long-term attention to digestive health.
Dietary Considerations
Patients may benefit from:
- Smaller, more frequent meals
- Avoiding spicy foods if symptoms worsen
- Limiting alcohol
- Reducing highly acidic foods when poorly tolerated
- Maintaining adequate hydration
Medication Awareness
Patients should discuss chronic use of:
- Aspirin
- NSAIDs
- Steroids
with their healthcare provider.
Monitoring Symptoms
Seek medical attention if any of the following occur:
- Vomiting blood
- Black stools
- Unintentional weight loss
- Persistent vomiting
- Severe abdominal pain
- Progressive anemia
Emotional and Quality-of-Life Impact
Chronic digestive symptoms can affect:
- Appetite
- Sleep
- Daily functioning
- Social activities
Working closely with a gastroenterologist can help optimize symptom control and prevent complications.
Key Differences Summary
| Feature | Gastritis | Gastropathy |
| Definition | Inflammation of gastric mucosa | Gastric mucosal injury without significant inflammation |
| Nature | Disease process | Morphological/histological description |
| Inflammatory Cells | Present | Minimal or absent |
| Common Causes | H. pylori, autoimmune disease, infections | NSAIDs, bile reflux, alcohol, portal hypertension |
| Histology | Inflammatory infiltrates | Epithelial injury and reactive changes |
| Cancer Risk | May increase in chronic cases | Usually lower unless associated with another disorder |
| Treatment Focus | Eliminate inflammation cause | Remove the source of mucosal injury. |
Conclusion
Although the terms are sometimes used interchangeably, gastritis and gastropathy are distinct entities with different pathological foundations. Accurate diagnosis, frequently requiring endoscopic biopsy, is essential because treatment strategies depend on identifying the underlying cause. Recognizing these differences enables clinicians to provide targeted therapy, reduce complications, and improve long-term gastrointestinal health and quality of life for affected patients.