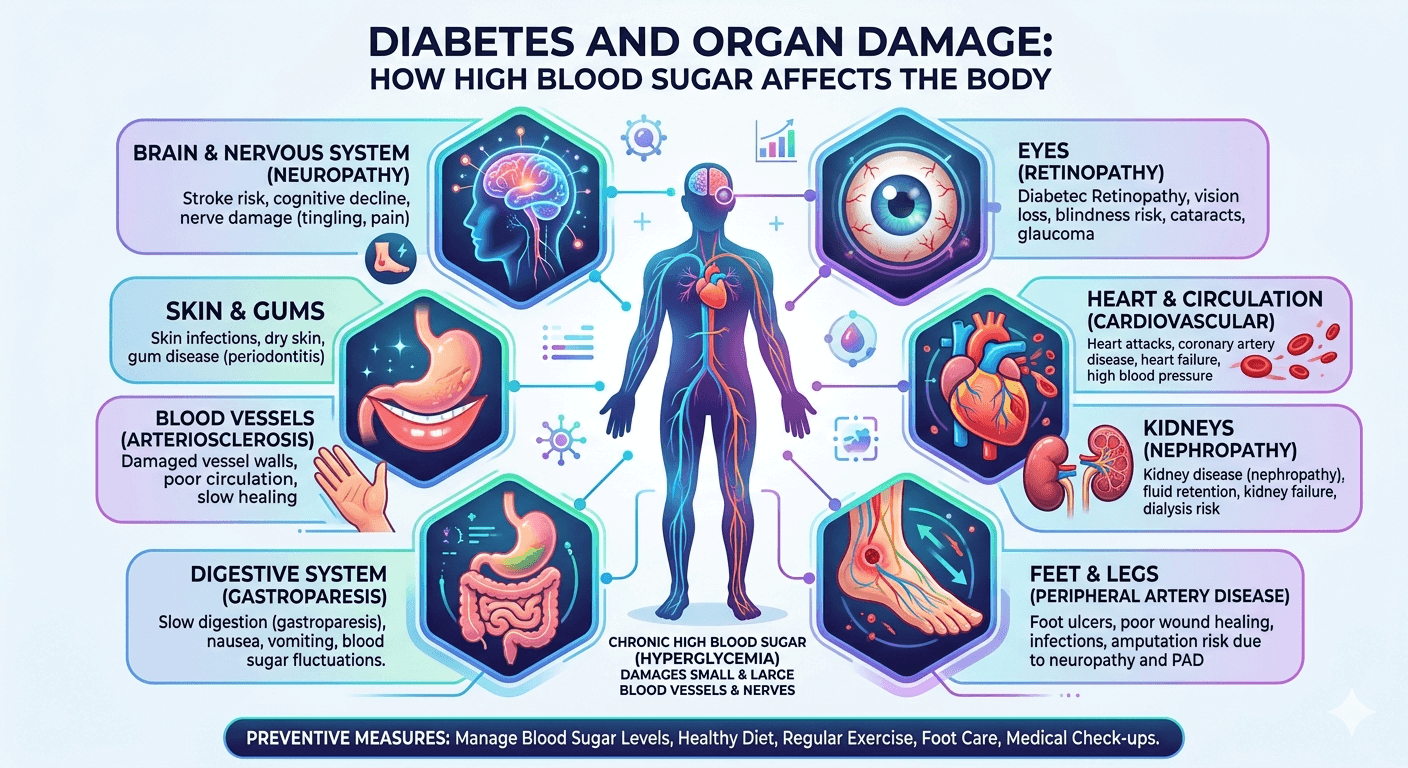
Diabetic neuropathy refers to nerve damage that occurs as a complication of diabetes, often due to long-term high blood sugar levels. It commonly affects peripheral nerves, resulting in symptoms like pain, tingling, numbness, and weakness, starting in the feet and hands. If untreated, it can lead to serious complications, such as infections, ulcers, or amputations. However, with proper care, the condition can be managed effectively.
Types of Diabetic Neuropathy
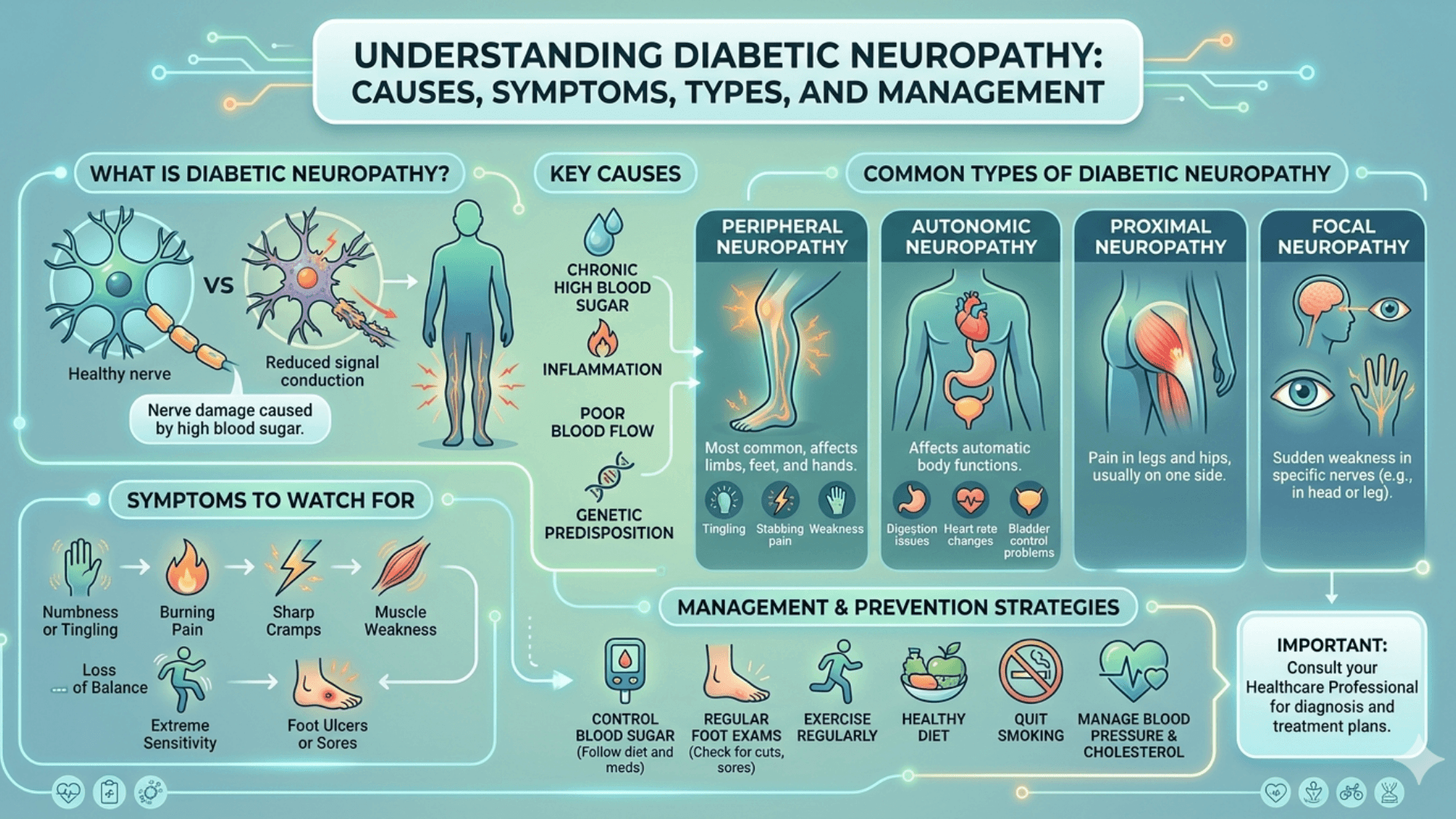
There are four primary forms of diabetic neuropathy:
Peripheral Neuropathy: This is the most common type, affecting the feet, legs, hands, and arms. It causes symptoms like tingling, numbness, and pain.
Autonomic Neuropathy: This impacts the nerves controlling involuntary body functions, such as heart rate and digestion. It can result in digestive issues, dizziness, and urinary problems.
Proximal Neuropathy: Also known as diabetic amyotrophy, this type causes pain and muscle weakness in the thighs, hips, or buttocks, usually on one side.
Focal Neuropathy: This involves sudden pain or weakness in specific nerves, often in the eyes or face, and tends to improve over time.
Causes of Diabetic Neuropathy
The primary factor behind diabetic neuropathy is high blood glucose levels, which damage blood vessels that nourish the nerves, leading to nerve dysfunction. Several contributing factors include:
Chronic High Blood Sugar: Consistently elevated blood sugar levels cause harmful substances to accumulate, damaging nerve fibers.
Inflammation: Ongoing inflammation due to diabetes can contribute to nerve damage.
Poor Circulation: Reduced blood flow due to high blood sugar levels deprives nerves of essential nutrients and oxygen.
Genetics: Some individuals may be more prone to developing neuropathy due to genetic factors.
Duration of Diabetes: The longer someone has diabetes, the higher their risk of developing neuropathy, especially if their blood sugar levels have been poorly managed.
Symptoms of Diabetic Neuropathy
The symptoms of diabetic neuropathy vary, but they commonly include:
Tingling or numbness in the hands, feet, or legs
Sharp or burning pain
Increased sensitivity to touch
Muscle weakness and poor coordination, especially in the feet and hands
Digestive problems such as nausea, constipation, and diarrhea (in autonomic neuropathy)
Urinary issues like incontinence or difficulty emptying the bladder
Dizziness or fainting due to low blood pressure upon standing
Managing Diabetic Neuropathy
Managing diabetic neuropathy involves controlling blood sugar levels and addressing symptoms to prevent further nerve damage. Key strategies include:
Blood Sugar Control: Keeping blood sugar within the target range through diet, exercise, and medication is crucial in preventing further nerve damage.
Pain Management: Medications like anti-seizure drugs (gabapentin) or antidepressants (amitriptyline) can help control pain and discomfort caused by nerve damage.
Physical Therapy: Physical therapy can improve strength and balance, particularly in cases of muscle weakness or coordination issues.
Foot Care: Regular foot inspections are vital, as nerve damage can prevent pain sensation, leading to unnoticed injuries and infections.
Lifestyle Adjustments: A balanced diet, regular physical activity, quitting smoking, and managing blood pressure and cholesterol are all essential for controlling the condition.
Surgical Options: In some cases, surgery may be needed to address specific issues caused by neuropathy, such as a compressed nerve.
Routine Monitoring: Regular doctor visits, blood tests, and foot exams are important for tracking the progression of the condition.
Precautions in Diabetic Neuropathy
Diabetic neuropathy is a nerve damage complication caused by prolonged high blood sugar levels. Proper precautions can help slow progression, reduce symptoms, and prevent serious complications.
Important Precautions
- Maintain good blood sugar control through regular monitoring and proper medication use.
- Inspect feet daily for cuts, blisters, redness, swelling, or ulcers.
- Wear comfortable, well-fitted footwear to avoid foot injuries.
- Avoid walking barefoot, even inside the house.
- Keep feet clean and moisturized, but avoid excess moisture between toes.
- Trim toenails carefully to prevent infections.
- Stop smoking and limit alcohol intake, as both worsen nerve damage and circulation.
- Exercise regularly to improve blood flow and nerve health.
- Maintain a healthy body weight.
- Attend regular medical checkups for blood sugar, kidney function, eye health, and nerve assessment.
- Avoid exposure to extreme heat or cold because reduced sensation may increase the risk of burns or injuries.
Diet Plan for Diabetic Neuropathy
A balanced diet helps control blood glucose levels and supports nerve function.
Foods to Include
- Whole grains such as oats, brown rice, quinoa, and whole wheat
- High-fiber vegetables like spinach, broccoli, carrots, and beans
- Fresh fruits in moderate portions, especially berries, apples, and guava
- Lean proteins including fish, eggs, chicken, tofu, and legumes
- Healthy fats from nuts, seeds, olive oil, and avocado
- Low-fat dairy products
- Foods rich in vitamin B12, vitamin D, magnesium, and omega-3 fatty acids
Foods to Avoid
- Sugary drinks and sweets
- Refined carbohydrates such as white bread and pastries
- Fried and processed foods
- Excess salt and packaged snacks
- Alcohol and smoking
- High-fat fast foods
Conclusion
Diabetic neuropathy is a serious condition that can lead to significant complications if not managed properly. Early detection and good blood sugar control are crucial for slowing its progression. With the right treatment plan and regular monitoring, those affected can manage their symptoms and maintain a better quality of life. A healthy diet combined with regular exercise, stress management, and proper diabetes control can significantly reduce the risk of worsening diabetic neuropathy.
Disclaimer: The information provided in this blog post is for educational and informational purposes only and should not be considered medical advice. It is not intended to replace professional medical consultation, diagnosis, or treatment.